Chiang Chi-Lu, Wang Lei-Chi, Ho Hsiang-Ling, Tsai Chun-Ming, Yeh Yi-Chen, Hsu Wen-Hu, Chou Teh-Ying, Chiu Chao-Hua, Wu Yu-Chung
Division of Thoracic Oncology, Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
Faculty of Medicine, School of Medicine, National Yang-Ming University, Taipei, Taiwan.
Oncotarget. 2017 Dec 26;9(4):5435-5444. doi: 10.18632/oncotarget.23686. eCollection 2018 Jan 12.
Occasionally, malignant pleural disease is only detected unexpectedly during surgery in patients with pulmonary adenocarcinoma. Previous studies mostly focused on the role of main tumor resection on patient's outcome, barely addressing the position of postoperative systemic therapy.
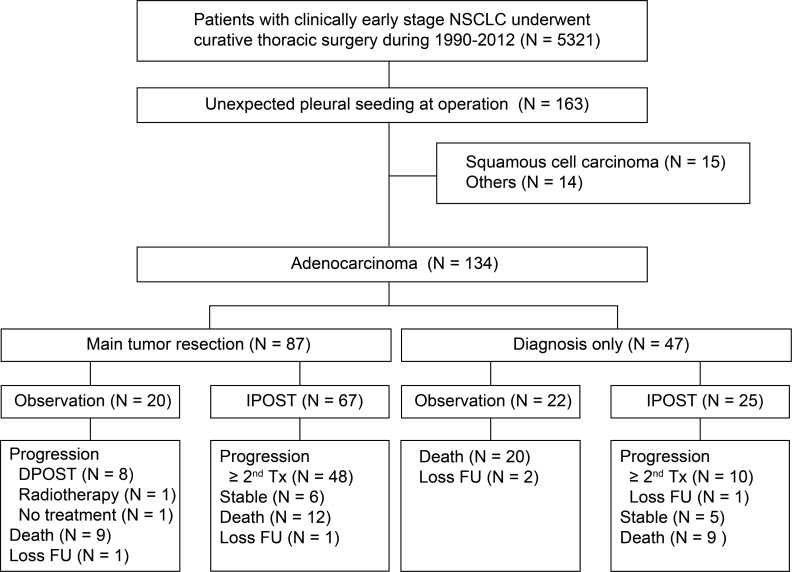
The medical records of 5321 non-small cell lung cancer patients who underwent thoracic surgery between January 1990 and December 2012 were reviewed. Pulmonary adenocarcinoma patients with unexpected pleural spread noted during surgery were included. The clinical and postoperative treatment variables were assessed for correlation with overall survival.
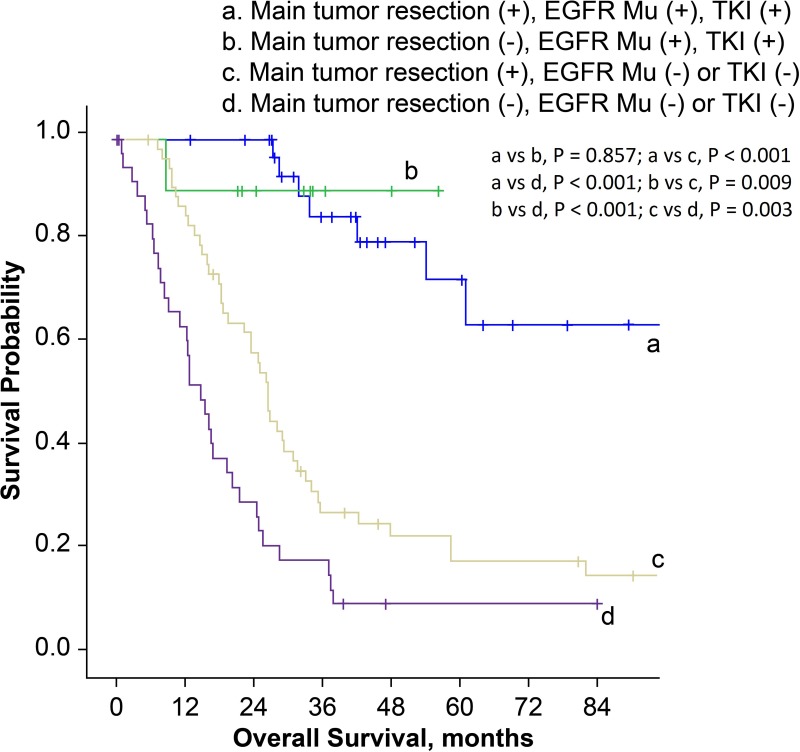
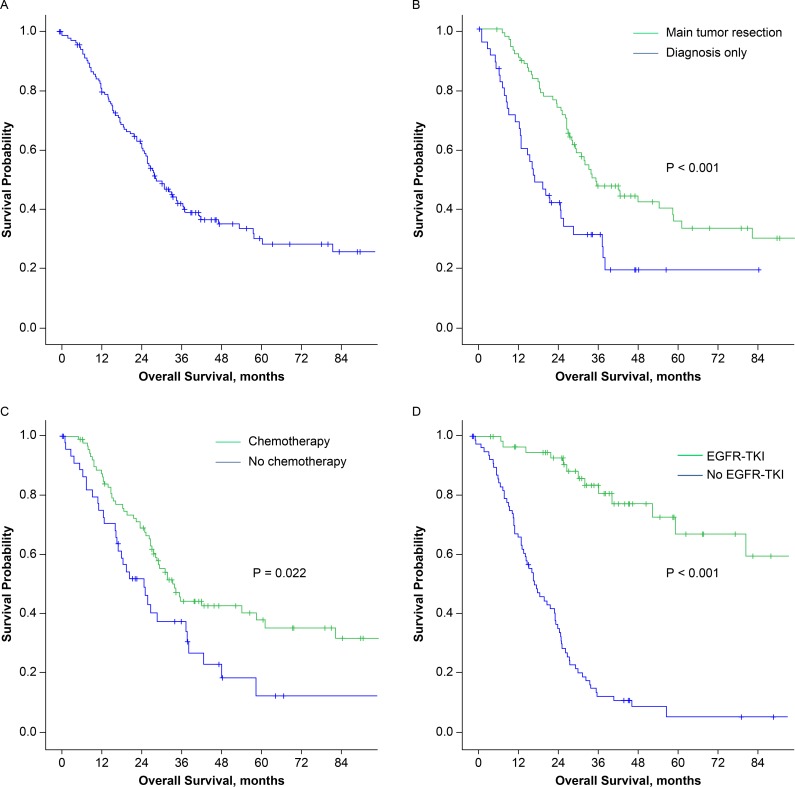
In 134 patients identified, main tumor resection was performed in 87 (64.9%) patients, while 89 (66.4%) and 57 (42.5%) patients received postoperative chemotherapy and epidermal growth factor receptor- tyrosine kinase inhibitor (EGFR -TKI) therapy, respectively. Overall, the 5-year survival rate was 30.2% and median survival time was 29.3 months. Multivariate analysis showed main tumor resection and EGFR-TKI therapy were associated with better survival. Mutational status of EGFR was available in 57 patients and 43 (75.4%) had activating mutations. Resection of the main tumor conferred a better outcome in patients without EGFR mutation or with unknown EGFR mutation status and had not been treated with EGFR-TKI therapy ( = 0.003), but not in those with activating EGFR mutation and had been treated with EGFR-TKI ( = 0.857).
In pulmonary adenocarcinoma patients with unexpected pleural spread detected during surgery, main tumor resection and EGFR-TKI therapy correlated with better survival. Identifying EGFR mutation status before surgery can provide useful information for clinical decision during surgery.
偶尔,恶性胸膜疾病仅在肺腺癌患者手术期间意外被发现。既往研究大多关注主肿瘤切除对患者预后的作用,几乎未涉及术后全身治疗的地位。
回顾了1990年1月至2012年12月期间接受胸外科手术的5321例非小细胞肺癌患者的病历。纳入手术期间发现意外胸膜转移的肺腺癌患者。评估临床和术后治疗变量与总生存期的相关性。
在确定的134例患者中,87例(64.9%)患者进行了主肿瘤切除,而分别有89例(66.4%)和57例(42.5%)患者接受了术后化疗和表皮生长因子受体-酪氨酸激酶抑制剂(EGFR-TKI)治疗。总体而言,5年生存率为30.2%,中位生存时间为29.3个月。多因素分析显示主肿瘤切除和EGFR-TKI治疗与更好的生存相关。57例患者可获得EGFR突变状态,其中43例(75.4%)有激活突变。对于未发生EGFR突变或EGFR突变状态未知且未接受EGFR-TKI治疗的患者,主肿瘤切除可带来更好的预后(P = 0.003),但对于发生EGFR激活突变且接受过EGFR-TKI治疗的患者则不然(P = 0.857)。
在手术期间发现意外胸膜转移的肺腺癌患者中,主肿瘤切除和EGFR-TKI治疗与更好的生存相关。术前确定EGFR突变状态可为手术期间的临床决策提供有用信息。