Yale School of Medicine, Department of Psychiatry, New Haven, CT (WR, SAM), and Yale School of Medicine, Department of Internal Medicine, New Haven, CT (JMS, JMT).
J Addict Med. 2018 May/Jun;12(3):227-233. doi: 10.1097/ADM.0000000000000392.
Heavy-drinking tobacco users are less likely to successfully quit smoking than their moderate-drinking counterparts, even when they are prescribed smoking cessation medication. One strategy for improving treatment outcomes in this subgroup of tobacco users may be to combine medication therapies to target both alcohol and tobacco use simultaneously. Adding naltrexone to frontline smoking cessation treatments may improve treatment outcomes in this group.
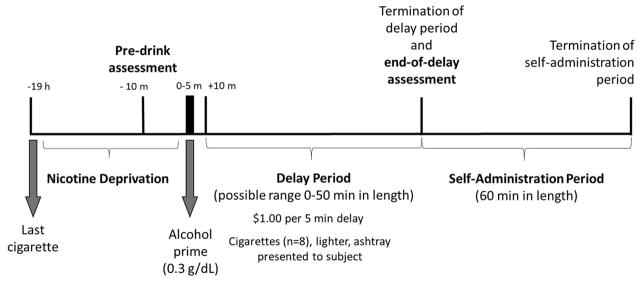
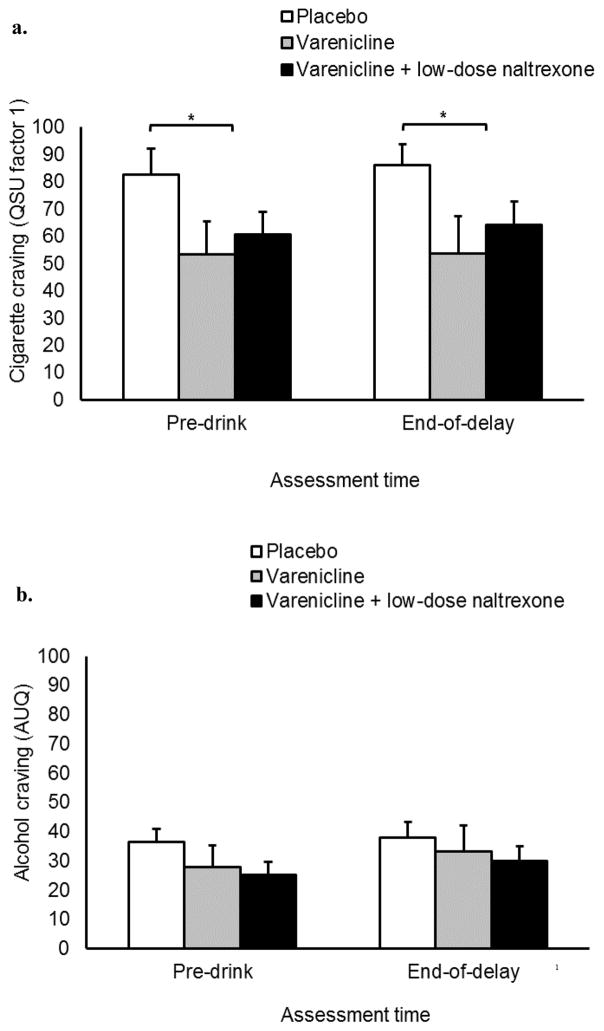
This double-blind, placebo-controlled human laboratory study examined the effects of varenicline (2 mg/d) and varenicline (2 mg/d), combined with a low dose of naltrexone (25 mg/d) on alcohol-primed smoking behavior in a laboratory model of smoking relapse in heavy-drinking tobacco users (n = 30). Participants attended a laboratory session and received an alcohol challenge (target breath alcohol concentration = 0.030 g/dL). They completed a smoking delay task that assessed their ability to resist smoking followed by an ad libitum smoking phase (primary outcomes). They also provided ratings of subjective drug effects and craving, and carbon monoxide levels were measured after smoking (secondary outcomes).
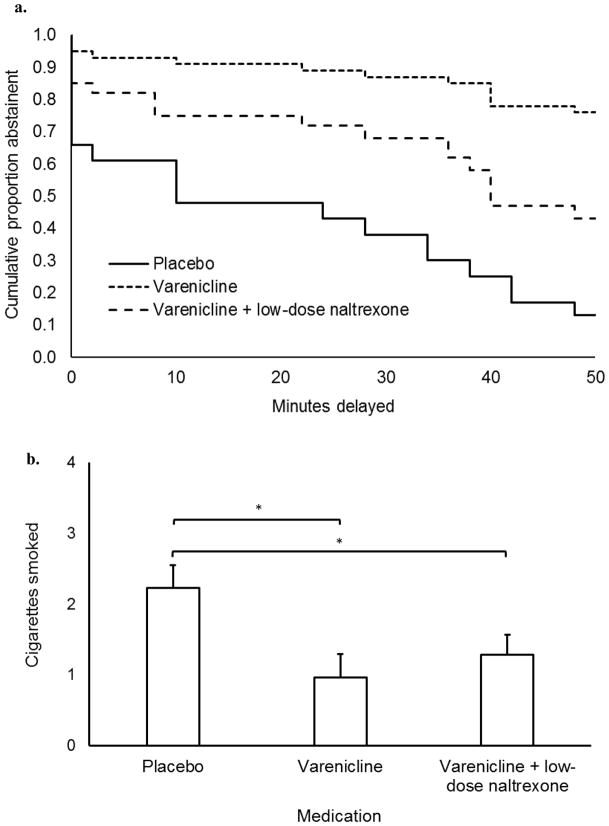
Participants receiving varenicline monotherapy delayed smoking longer and smoked fewer cigarettes than those on placebo. Participants receiving varenicline + low-dose naltrexone did not delay smoking longer than those receiving varenicline alone. Participants in both active medication arms smoked fewer cigarettes ad libitum than those receiving placebo.
Varenicline can improve smoking outcomes even after an alcohol prime, supporting its use in heavy drinkers who wish to quit smoking. Findings did not support increased efficacy of combined varenicline + low-dose naltrexone relative to varenicline monotherapy.
重度饮酒烟草使用者成功戒烟的可能性低于适度饮酒者,即使他们被开了戒烟药物。改善这组烟草使用者治疗效果的一种策略可能是将药物治疗联合起来,同时针对酒精和烟草使用。在一线戒烟治疗中加入纳曲酮可能会改善这一人群的治疗效果。
这项双盲、安慰剂对照的人体实验室研究,考察了在重度饮酒烟草使用者的实验室吸烟复吸模型中,伐伦克林(2mg/d)和伐伦克林(2mg/d)联合低剂量纳曲酮(25mg/d)对酒精诱发吸烟行为的影响(n=30)。参与者参加了一个实验室会议,并接受了酒精挑战(目标呼气酒精浓度=0.030g/dL)。他们完成了一个延迟吸烟任务,评估他们抵抗吸烟的能力,然后进行自由吸烟阶段(主要结果)。他们还提供了药物主观效应和渴求的评分,并且在吸烟后测量了一氧化碳水平(次要结果)。
接受伐伦克林单药治疗的参与者比接受安慰剂的参与者延迟吸烟时间更长,吸烟量更少。接受伐伦克林+低剂量纳曲酮治疗的参与者与接受伐伦克林单药治疗的参与者相比,并没有延长吸烟时间。接受两种活性药物治疗的参与者与接受安慰剂的参与者相比,自由吸烟时吸烟量更少。
即使在酒精激发后,伐伦克林也可以改善吸烟结果,支持其在希望戒烟的重度饮酒者中的使用。结果不支持联合伐伦克林+低剂量纳曲酮相对于伐伦克林单药治疗的疗效增加。