Chamie Gabriel, Kato-Maeda Midori, Emperador Devy M, Wandera Bonnie, Mugagga Olive, Crandall John, Janes Michael, Marquez Carina, Kamya Moses R, Charlebois Edwin D, Havlir Diane V
Division of HIV, Infectious Diseases and Global Medicine, University of California, San Francisco, California, United States of America.
Curry International Tuberculosis Center, Division of Pulmonary and Critical Care Medicine, University of California, San Francisco, United States of America.
PLoS One. 2018 Feb 13;13(2):e0192666. doi: 10.1371/journal.pone.0192666. eCollection 2018.
Incomplete understanding of TB transmission dynamics in high HIV prevalence settings remains an obstacle for prevention. Understanding where transmission occurs could provide a platform for case finding and interrupting transmission.
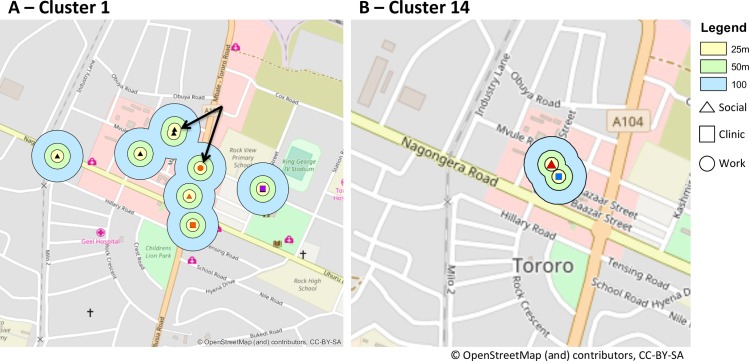
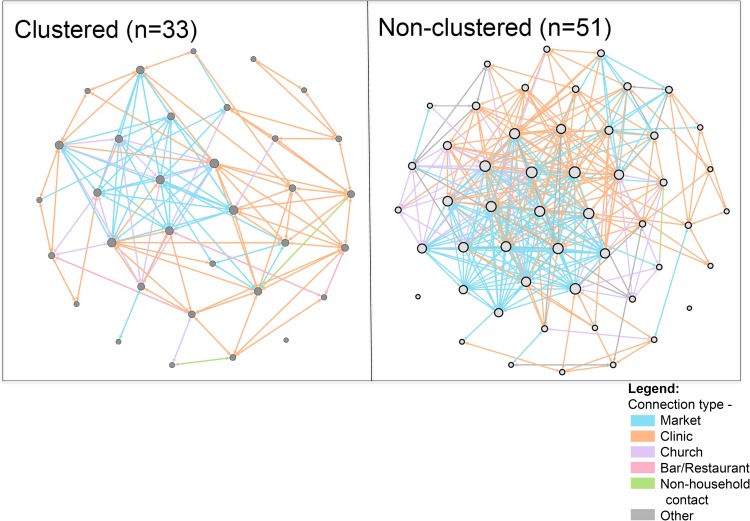
From 2012-2015, we sought to recruit all adults starting TB treatment in a Ugandan community. Participants underwent household (HH) contact investigation, and provided names of social contacts, sites of work, healthcare and socializing, and two sputum samples. Mycobacterium tuberculosis culture-positive specimens underwent 24-loci MIRU-VNTR and spoligotyping. We sought to identify epidemiologic links between genotype-matched cases by analyzing social networks and mapping locations where cases reported spending ≥12 hours over the one-month pre-treatment. Sites of spatial overlap (≤100m) between genotype-matched cases were considered potential transmission sites. We analyzed social networks stratified by genotype clustering status, with cases linked by shared locations, and compared network density by location type between clustered vs. non-clustered cases.
Of 173 adults with TB, 131 (76%) were enrolled, 108 provided sputum, and 84/131 (78%) were MTB culture-positive: 52% (66/131) tested HIV-positive. Of 118 adult HH contacts, 105 (89%) were screened and 3 (2.5%) diagnosed with active TB. Overall, 33 TB cases (39%) belonged to 15 distinct MTB genotype-matched clusters. Within each cluster, no cases shared a HH or reported shared non-HH contacts. In 6/15 (40%) clusters, potential epidemiologic links were identified by spatial overlap at specific locations: 5/6 involved health care settings. Genotype-clustered TB social networks had significantly greater network density based on shared clinics (p<0.001) and decreased density based on shared marketplaces (p<0.001), compared to non-clustered networks.
In this molecular epidemiologic study, links between MTB genotype-matched cases were only identifiable via shared locations, healthcare locations in particular, rather than named contacts. This suggests most transmission is occurring between casual contacts, and emphasizes the need for improved infection control in healthcare settings in rural Africa.
在艾滋病毒高流行地区,对结核病传播动态的不完全了解仍然是预防工作的障碍。了解传播发生的地点可为病例发现和阻断传播提供一个平台。
2012年至2015年期间,我们试图招募乌干达一个社区中所有开始接受结核病治疗的成年人。参与者接受了家庭接触者调查,并提供了社会接触者的姓名、工作地点、医疗保健和社交场所,以及两份痰标本。结核分枝杆菌培养阳性标本进行了24位点MIRU-VNTR和间隔寡核苷酸分型。我们试图通过分析社交网络并绘制病例报告在治疗前一个月内花费≥12小时的地点,来确定基因型匹配病例之间的流行病学联系。基因型匹配病例之间空间重叠(≤100米)的地点被视为潜在传播地点。我们按基因型聚类状态对社交网络进行分层分析,病例通过共享地点建立联系,并比较聚类病例与非聚类病例按地点类型划分的网络密度。
在173名结核病成人患者中,131名(76%)被纳入研究,108名提供了痰标本,84/131(78%)结核分枝杆菌培养阳性:52%(66/131)检测出艾滋病毒阳性。在118名成年家庭接触者中,105名(89%)接受了筛查,3名(2.5%)被诊断为活动性结核病。总体而言,33例结核病病例(39%)属于15个不同的结核分枝杆菌基因型匹配聚类。在每个聚类中,没有病例共享一个家庭或报告有共享的非家庭接触者。在6/15(40%)个聚类中,通过特定地点的空间重叠确定了潜在的流行病学联系:5/6涉及医疗保健场所。与非聚类网络相比,基于共享诊所的基因型聚类结核病社交网络的网络密度显著更高(p<0.001),而基于共享市场的网络密度则降低(p<0.001)。
在这项分子流行病学研究中,结核分枝杆菌基因型匹配病例之间的联系只能通过共享地点,特别是医疗保健地点来确定,而不是通过指名的接触者。这表明大多数传播发生在偶然接触者之间,并强调了在非洲农村地区的医疗保健场所改善感染控制的必要性。