Department of Neurology, National Cerebral and Cardiovascular Center, Japan.
J Alzheimers Dis. 2018;62(1):61-72. doi: 10.3233/JAD-170970.
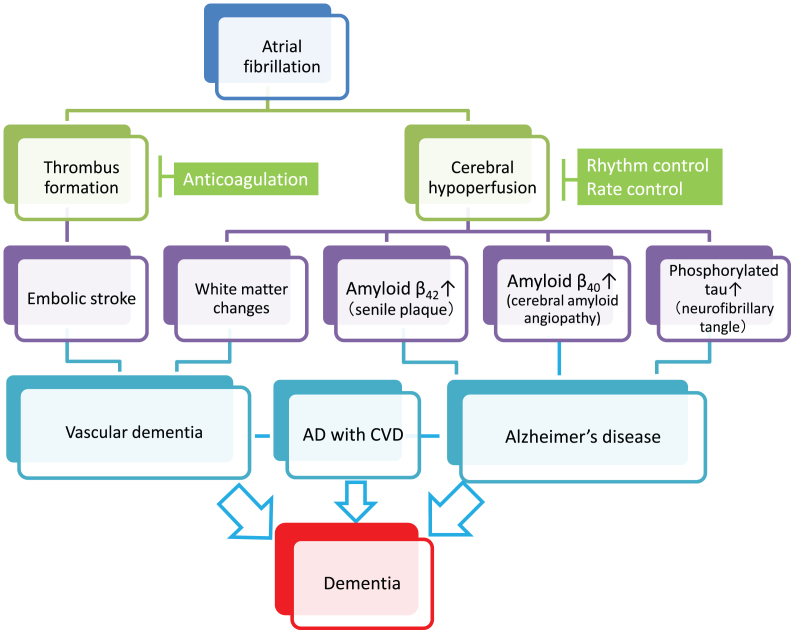
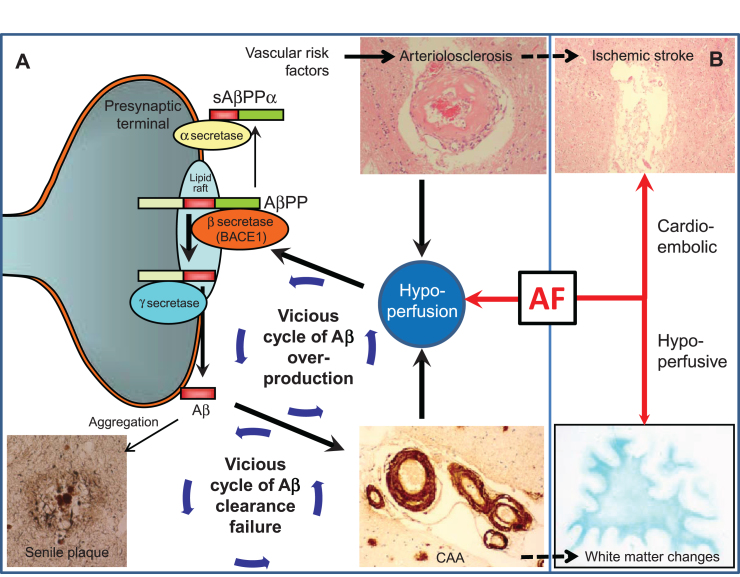
Many studies have shown a relationship between atrial fibrillation (AF) and vascular dementia. AF is a major risk factor for stroke, and stroke is the greatest risk factor for vascular dementia. However, the relationship between Alzheimer's disease (AD), the leading cause of dementia, and AF remains unclear. At least four epidemiological studies have reported AF significantly raises the risk of AD 1.5- to 2.5-fold. Chronic cerebral hypoperfusion, resulting from persistent AF, could explain the link as hypoperfusion may mechanistically exacerbate amyloid-β (Aβ) neuropathology, such as senile plaques and amyloid angiopathy, by upregulating Aβ-producing enzymes and lowering Aβ clearance efficiency. In addition, hypoperfusion may exacerbate tau pathology directly through upregulation of tau-phosphorylating enzymes and indirectly via the amyloid cascade. However, most neuropathological studies do not support the direct link between AD pathology and AF but rather suggests vascular neuropathology is related to, or coexistent with, AF and lowers the threshold for clinically-evident AD. Vascular neuropathology may thus mediate the link between AD and AF. From a treatment perspective, an observational study has shown that catheter ablation is associated with less incidence of AD in AF patients, suggesting rhythm-control suppresses hypoperfusion-induced AD neuropathology. In addition, rate-control may lower the rate of cognitive decline in cognitively impaired elderly subjects with AF. Further studies are warranted to clarify the mechanisms underlying the linkage between AF and AD. However, anticoagulation and rhythm-/rate-control against AF may hold promise even for AD patients.
许多研究表明心房颤动(AF)与血管性痴呆之间存在关联。AF 是中风的主要危险因素,而中风是血管性痴呆的最大危险因素。然而,阿尔茨海默病(AD)——痴呆的主要病因与 AF 之间的关系尚不清楚。至少有四项流行病学研究报告称,AF 使 AD 的风险增加 1.5-2.5 倍。持续性 AF 引起的慢性脑灌注不足可能可以解释这种关联,因为灌注不足可能通过上调β淀粉样蛋白(Aβ)产生酶和降低 Aβ清除效率,从而在机制上加重 Aβ神经病理学,例如老年斑和淀粉样血管病。此外,灌注不足可能通过上调tau 磷酸化酶直接加重 tau 病理学,并通过淀粉样蛋白级联反应间接加重。然而,大多数神经病理学研究并不支持 AD 病理学与 AF 之间的直接联系,而是表明血管性神经病理学与 AF 相关或并存,并降低了临床上明显 AD 的阈值。因此,血管性神经病理学可能介导了 AD 和 AF 之间的联系。从治疗角度来看,一项观察性研究表明,导管消融与 AF 患者中 AD 的发病率较低相关,这表明节律控制可抑制灌注不足引起的 AD 神经病理学。此外,节律控制可能会降低伴有 AF 的认知障碍老年患者认知能力下降的速度。需要进一步的研究来阐明 AF 和 AD 之间关联的机制。然而,即使对于 AD 患者,抗凝和针对 AF 的节律/速率控制也可能具有前景。