Nomura Hidetaka, Sakamoto Kimihiko, Sugihara Takeru, Okamoto Shuhei, Aoki Yoichi, Tanigawa Terumi, Matoda Maki, Omatsu Kohei, Kanao Hiroyuki, Kato Kazuyoshi, Utsugi Kuniko, Sugiyama Yuko, Takeshima Nobuhiro
Department of Gynecology, Cancer Institute Hospital Department of Obstetrics and Gynecology, NTT Medical Center, Tokyo, Japan.
Medicine (Baltimore). 2018 Feb;97(7):e9932. doi: 10.1097/MD.0000000000009932.
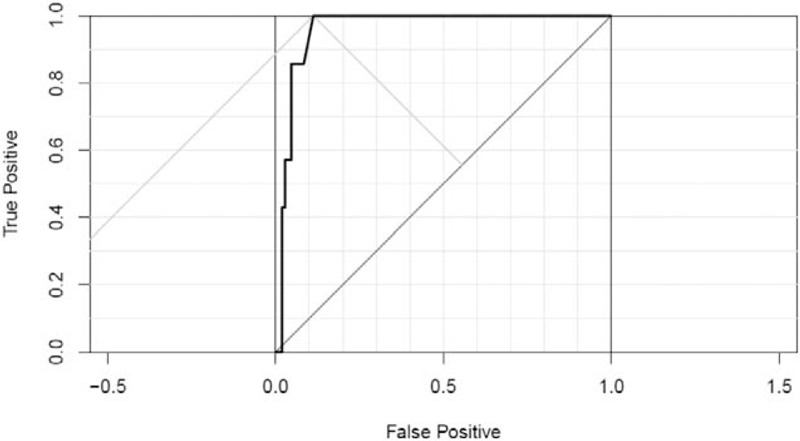
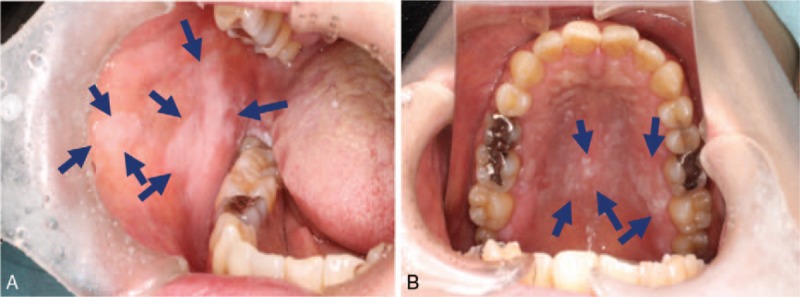
Pegylated liposomal doxorubicin (PLD) has a good safety profile, but long-term use has been associated with development of squamous cell carcinoma of the tongue and oral cavity (SCCTO) in some patients. The study objective was to estimate the prevalence of oral leukoplakia, a known precursor of SCCTO, in patients with ovarian cancer and long-term PLD use.After approval of the institutional review board, medical record of 114 patients who were treated with PLD at our institution between January 2010 and December 2016 were retrospectively reviewed. All those patients have been referred for routine monitoring of oral mucositis every time before administration by a dentist. The patient characteristics included in the evaluation were age, smoking and drinking habits, the PLD dose and schedule, and presence or absence of oral leukoplakia and SCCTO at each oral examination. The relationships of the incidence of oral leukoplakia and patient characteristics were analyzed.The median total PLD dose was 160 (range 40-1550) mg/m. Oral leukoplakia was seen in 6 (5.3%) patients. The median PLD dose, at the time of oral leukoplakia diagnosis, was 685 (range 400-800) mg/m. SCCTO was not found. Univariate analysis revealed that age, Brinkman index, and habitual drinking were not considered as risk factors for oral leukoplakia, and only total PLD dose (OR, 1.470; 95% CI, 1.19-1.91; P < .001) remained as a significant independent risk factor for oral leukoplakia. The ROC curve analysis indicated that the optimal cutoff value of the total PLD dose to predict development of oral leukoplakia was 400 mg/m. The sensitivity was 100% and the specificity was 88.8%. No patient discontinued PLD because of oral leukoplakia or SCCTO.The 2 most important clinical observations were the occurrence of oral leukoplakia in patients with long-term PLD use and that the development of oral leukoplakia was related to a total cumulative dose ≥400 mg/m. Routine oral surveillance is recommended, particularly when the cumulative total dose exceeds 400 mg/m.
聚乙二醇化脂质体阿霉素(PLD)具有良好的安全性,但在一些患者中,长期使用与舌和口腔鳞状细胞癌(SCCTO)的发生有关。本研究的目的是评估卵巢癌患者且长期使用PLD者中口腔白斑(SCCTO的已知前驱病变)的患病率。经机构审查委员会批准,对2010年1月至2016年12月期间在我院接受PLD治疗的114例患者的病历进行回顾性分析。每次给药前,所有这些患者均已被转介给牙医进行口腔黏膜炎的常规监测。评估中纳入的患者特征包括年龄、吸烟和饮酒习惯、PLD剂量和给药方案,以及每次口腔检查时口腔白斑和SCCTO的有无。分析口腔白斑发病率与患者特征之间的关系。PLD总剂量中位数为160(范围40 - 1550)mg/m²。6例(5.3%)患者出现口腔白斑。口腔白斑诊断时的PLD剂量中位数为685(范围400 - 800)mg/m²。未发现SCCTO。单因素分析显示,年龄、布林克曼指数和习惯性饮酒未被视为口腔白斑的危险因素,只有PLD总剂量(OR,1.470;95%CI,1.19 - 1.91;P <.001)仍然是口腔白斑的显著独立危险因素。ROC曲线分析表明,预测口腔白斑发生的PLD总剂量的最佳截断值为400mg/m²。敏感性为100%,特异性为88.8%。没有患者因口腔白斑或SCCTO而停用PLD。两项最重要的临床观察结果是长期使用PLD的患者出现口腔白斑,以及口腔白斑的发生与累积总剂量≥400mg/m²有关。建议进行常规口腔监测,尤其是当累积总剂量超过400mg/m²时。