Nordell Anna D, McKenna Matthew, Borges Álvaro H, Duprez Daniel, Neuhaus Jacqueline, Neaton James D
Division of Biostatistics, School of Public Health, University of Minnesota, Minneapolis, MN (A.D.N., M.M.K., J.N., J.D.N.).
Department of Infectious Diseases, Rigshospitalet and Copenhagen HIV Programme, University of Copenhagen, Copenhagen, Denmark (B.).
J Am Heart Assoc. 2014 May 28;3(3):e000844. doi: 10.1161/JAHA.114.000844.
In the general population, raised levels of inflammatory markers are stronger predictors of fatal than nonfatal cardiovascular disease (CVD) events. People with HIV have elevated levels of interleukin-6 (IL-6), high-sensitivity C-reactive protein (hsCRP), and D-dimer; HIV-induced activation of inflammatory and coagulation pathways may be responsible for their greater risk of CVD. Whether the enhanced inflammation and coagulation associated with HIV is associated with more fatal CVD events has not been investigated.
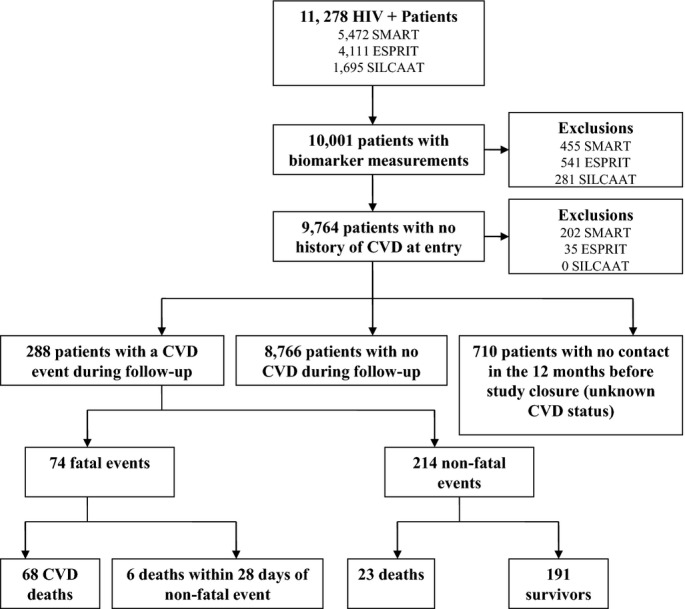
Biomarkers were measured at baseline for 9764 patients with HIV and no history of CVD. Of these patients, we focus on the 288 that experienced either a fatal (n=74) or nonfatal (n=214) CVD event over a median of 5 years. Odds ratios (ORs) (fatal versus nonfatal CVD) (95% confidence intervals [CIs]) associated with a doubling of IL-6, D-dimer, hsCRP, and a 1-unit increase in an IL-6 and D-dimer score, measured a median of 2.6 years before the event, were 1.39 (1.07 to 1.79), 1.40 (1.10 to 1.78), 1.09 (0.93 to 1.28), and 1.51 (1.15 to 1.97), respectively. Of the 214 patients with nonfatal CVD, 23 died during follow-up. Hazard ratios (95% CI) for all-cause mortality were 1.72 (1.28 to 2.31), 1.73 (1.27 to 2.36), 1.44 (1.15 to 1.80), and 1.88 (1.39 to 2.55), respectively, for IL-6, D-dimer, hsCRP, and the IL-6 and D-dimer score.
Higher IL-6 and D-dimer levels reflecting enhanced inflammation and coagulation associated with HIV are associated with a greater risk of fatal CVD and a greater risk of death after a nonfatal CVD event.
http://www.clinicaltrial.gov Unique identifier: SMART: NCT00027352, ESPRIT: NCT00004978, SILCAAT: NCT00013611.
在普通人群中,炎症标志物水平升高对致命性心血管疾病(CVD)事件的预测能力强于非致命性CVD事件。HIV感染者的白细胞介素-6(IL-6)、高敏C反应蛋白(hsCRP)和D-二聚体水平升高;HIV诱导的炎症和凝血途径激活可能是其CVD风险增加的原因。与HIV相关的炎症和凝血增强是否与更多致命性CVD事件相关尚未得到研究。
对9764例无CVD病史的HIV患者在基线时进行生物标志物检测。在这些患者中,我们重点关注在中位5年期间发生致命性(n = 74)或非致命性(n = 214)CVD事件的288例患者。事件发生前中位2.6年时,IL-6、D-二聚体、hsCRP水平翻倍以及IL-6和D-二聚体评分增加1个单位与致命性CVD(而非致命性CVD)相关的比值比(OR)(95%置信区间[CI])分别为1.39(1.07至1.79)、1.40(1.10至1.78)、1.09(0.93至1.28)和1.51(1.15至1.97)。在214例非致命性CVD患者中,23例在随访期间死亡。IL-6、D-二聚体、hsCRP以及IL-6和D-二聚体评分的全因死亡率风险比(95%CI)分别为1.72(1.28至2.31)、1.73(1.27至2.36)、1.44(1.15至1.80)和1.88(1.39至2.55)。
反映与HIV相关的炎症和凝血增强的较高IL-6和D-二聚体水平与致命性CVD风险增加以及非致命性CVD事件后死亡风险增加相关。
http://www.clinicaltrial.gov 唯一标识符:SMART:NCT00027352,ESPRIT:NCT00004978,SILCAAT:NCT00013611。