From the Diabetes and Cardiovascular Research Center (G.J., J.R.S.) and Department of Medical Pharmacology and Physiology (M.A.H., J.R.S.), University of Missouri School of Medicine, Columbia; Dalton Cardiovascular Research Center, University of Missouri, Columbia (M.A.H., J.R.S.); and Research Service, Truman Memorial Veterans Hospital, Columbia, MO (G.J., J.R.S.).
Circ Res. 2018 Feb 16;122(4):624-638. doi: 10.1161/CIRCRESAHA.117.311586.
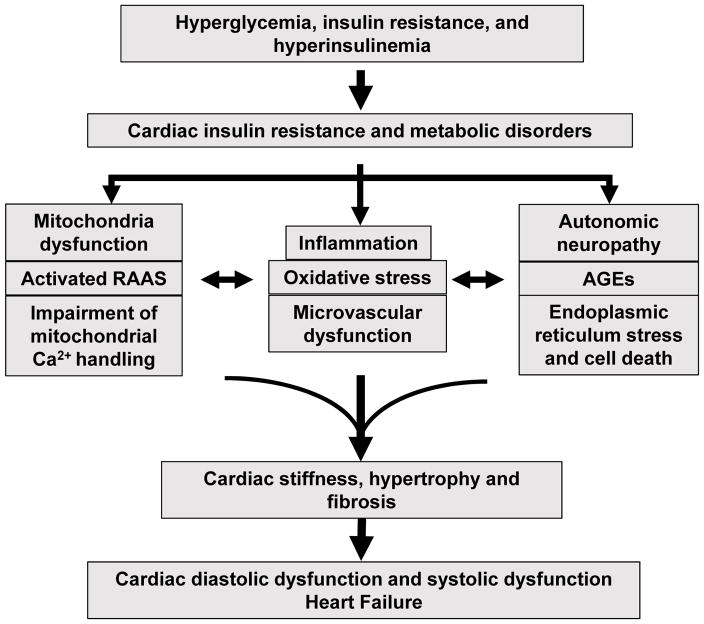
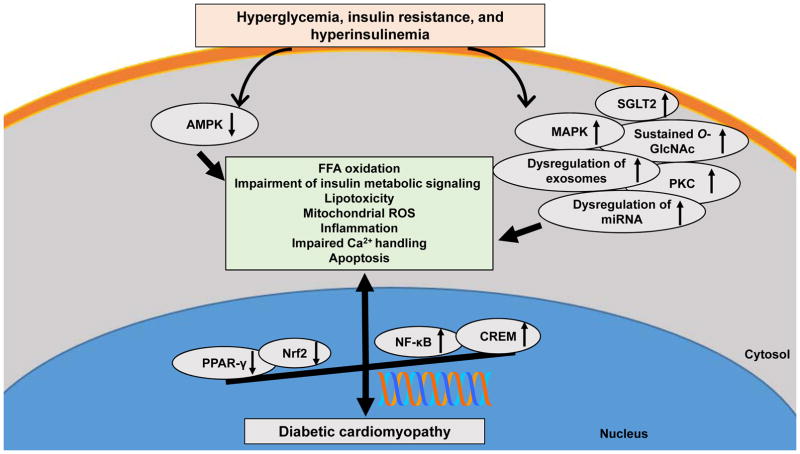
Heart failure and related morbidity and mortality are increasing at an alarming rate, in large part, because of increases in aging, obesity, and diabetes mellitus. The clinical outcomes associated with heart failure are considerably worse for patients with diabetes mellitus than for those without diabetes mellitus. In people with diabetes mellitus, the presence of myocardial dysfunction in the absence of overt clinical coronary artery disease, valvular disease, and other conventional cardiovascular risk factors, such as hypertension and dyslipidemia, has led to the descriptive terminology, diabetic cardiomyopathy. The prevalence of diabetic cardiomyopathy is increasing in parallel with the increase in diabetes mellitus. Diabetic cardiomyopathy is initially characterized by myocardial fibrosis, dysfunctional remodeling, and associated diastolic dysfunction, later by systolic dysfunction, and eventually by clinical heart failure. Impaired cardiac insulin metabolic signaling, mitochondrial dysfunction, increases in oxidative stress, reduced nitric oxide bioavailability, elevations in advanced glycation end products and collagen-based cardiomyocyte and extracellular matrix stiffness, impaired mitochondrial and cardiomyocyte calcium handling, inflammation, renin-angiotensin-aldosterone system activation, cardiac autonomic neuropathy, endoplasmic reticulum stress, microvascular dysfunction, and a myriad of cardiac metabolic abnormalities have all been implicated in the development and progression of diabetic cardiomyopathy. Molecular mechanisms linked to the underlying pathophysiological changes include abnormalities in AMP-activated protein kinase, peroxisome proliferator-activated receptors, O-linked N-acetylglucosamine, protein kinase C, microRNA, and exosome pathways. The aim of this review is to provide a contemporary view of these instigators of diabetic cardiomyopathy, as well as mechanistically based strategies for the prevention and treatment of diabetic cardiomyopathy.
心力衰竭及其相关发病率和死亡率正以惊人的速度增长,在很大程度上是由于人口老龄化、肥胖和糖尿病的增加。与没有糖尿病的患者相比,患有糖尿病的心力衰竭患者的临床结局要差得多。在患有糖尿病的人群中,即使没有明显的临床冠状动脉疾病、瓣膜疾病和其他传统心血管危险因素(如高血压和血脂异常),心肌功能障碍的存在也导致了一个描述性术语,即糖尿病性心肌病。随着糖尿病发病率的增加,糖尿病性心肌病的患病率也在增加。糖尿病性心肌病最初的特征是心肌纤维化、功能失调的重塑和相关的舒张功能障碍,随后是收缩功能障碍,最终发展为临床心力衰竭。心脏胰岛素代谢信号转导受损、线粒体功能障碍、氧化应激增加、一氧化氮生物利用度降低、晚期糖基化终产物和基于胶原蛋白的心肌细胞和细胞外基质硬度增加、线粒体和心肌细胞钙处理受损、炎症、肾素-血管紧张素-醛固酮系统激活、心脏自主神经病变、内质网应激、微血管功能障碍以及无数心脏代谢异常都与糖尿病性心肌病的发生和发展有关。与潜在病理生理变化相关的分子机制包括 AMP 激活的蛋白激酶、过氧化物酶体增殖物激活受体、O-连接的 N-乙酰葡萄糖胺、蛋白激酶 C、microRNA 和外泌体途径的异常。本文综述的目的是提供对这些糖尿病性心肌病诱发因素的现代观点,以及基于机制的预防和治疗糖尿病性心肌病的策略。