National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland.
National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland.
JACC Cardiovasc Imaging. 2018 May;11(5):697-707. doi: 10.1016/j.jcmg.2018.01.005. Epub 2018 Feb 14.
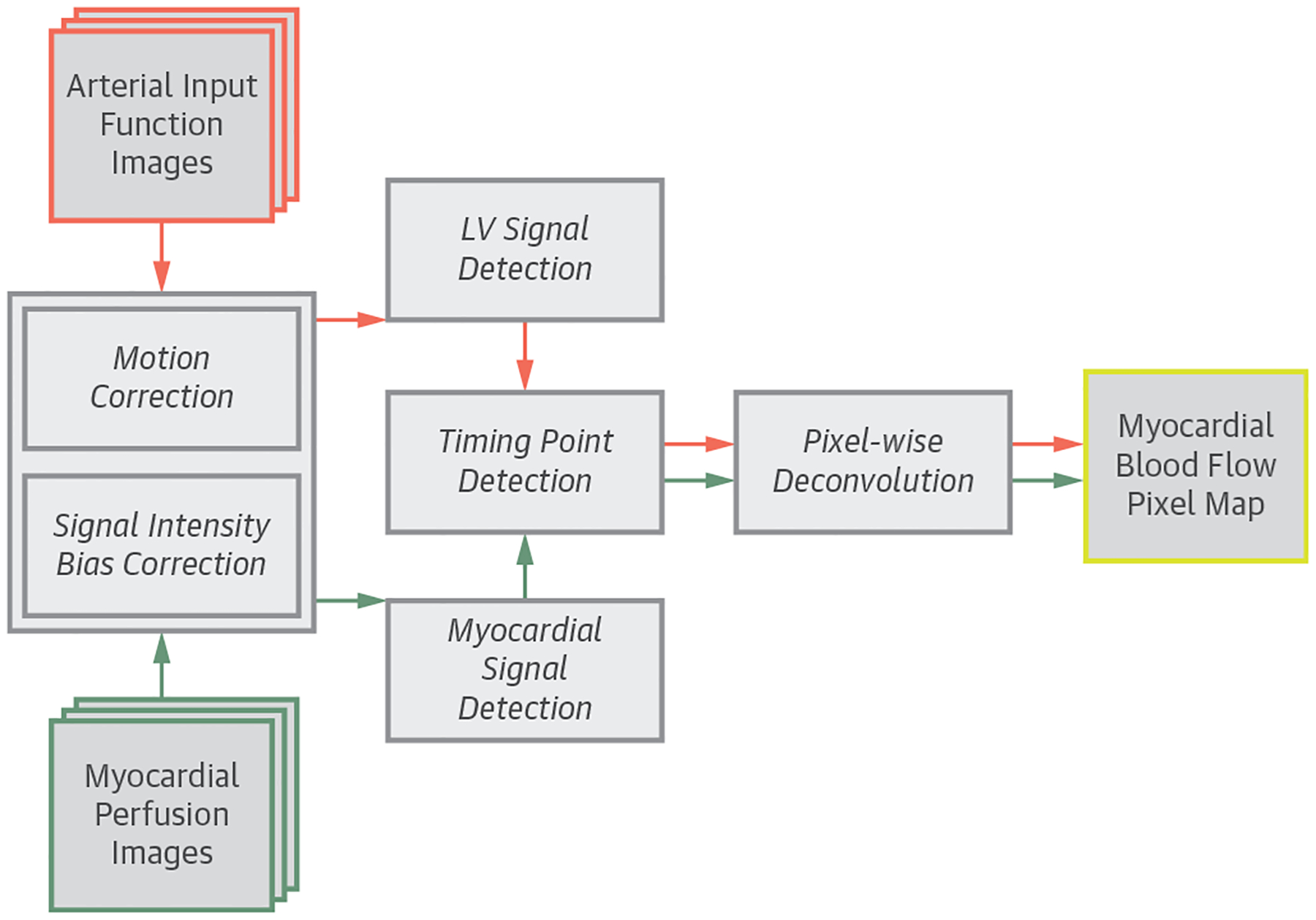
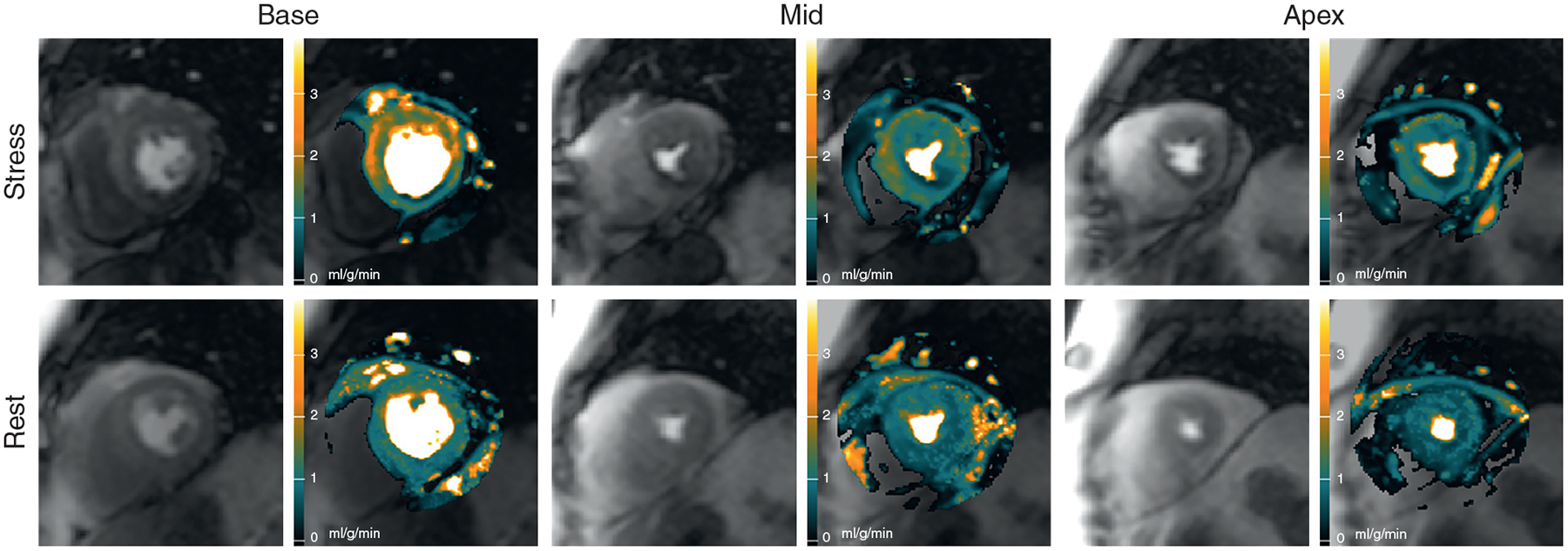
The authors developed a fully automated framework to quantify myocardial blood flow (MBF) from contrast-enhanced cardiac magnetic resonance (CMR) perfusion imaging and evaluated its diagnostic performance in patients.
Fully quantitative CMR perfusion pixel maps were previously validated with microsphere MBF measurements and showed potential in clinical applications, but the methods required laborious manual processes and were excessively time-consuming.
CMR perfusion imaging was performed on 80 patients with known or suspected coronary artery disease (CAD) and 17 healthy volunteers. Significant CAD was defined by quantitative coronary angiography (QCA) as ≥70% stenosis. Nonsignificant CAD was defined by: 1) QCA as <70% stenosis; or 2) coronary computed tomography angiography as <30% stenosis and a calcium score of 0 in all vessels. Automatically generated MBF maps were compared with manual quantification on healthy volunteers. Diagnostic performance of the automated MBF pixel maps was analyzed on patients using absolute MBF, myocardial perfusion reserve (MPR), and relative measurements of MBF and MPR.
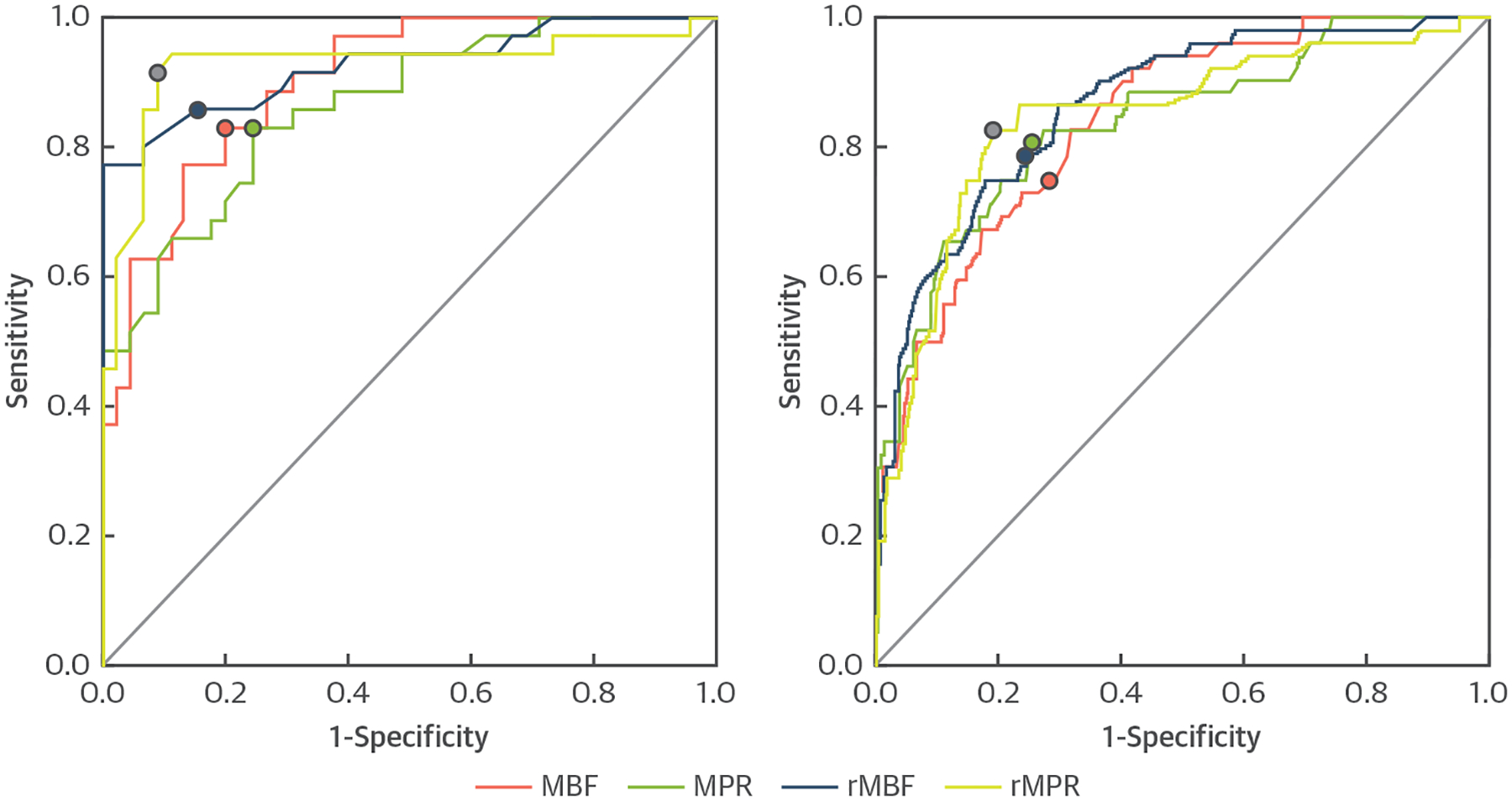
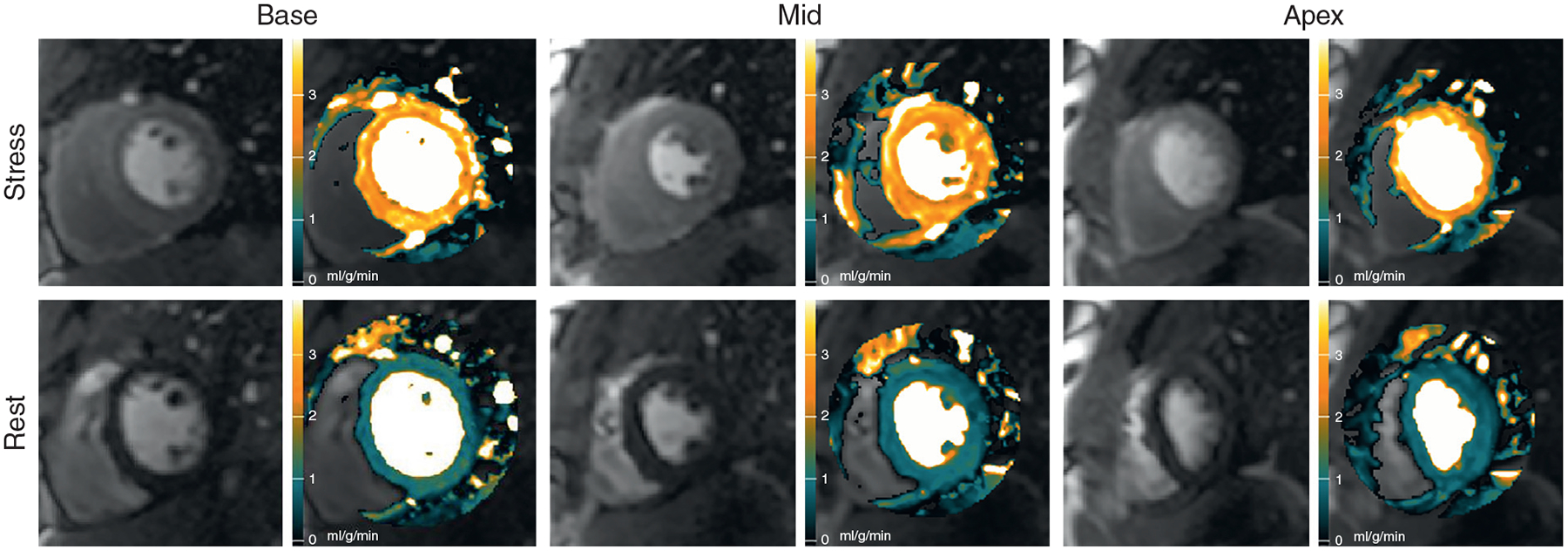
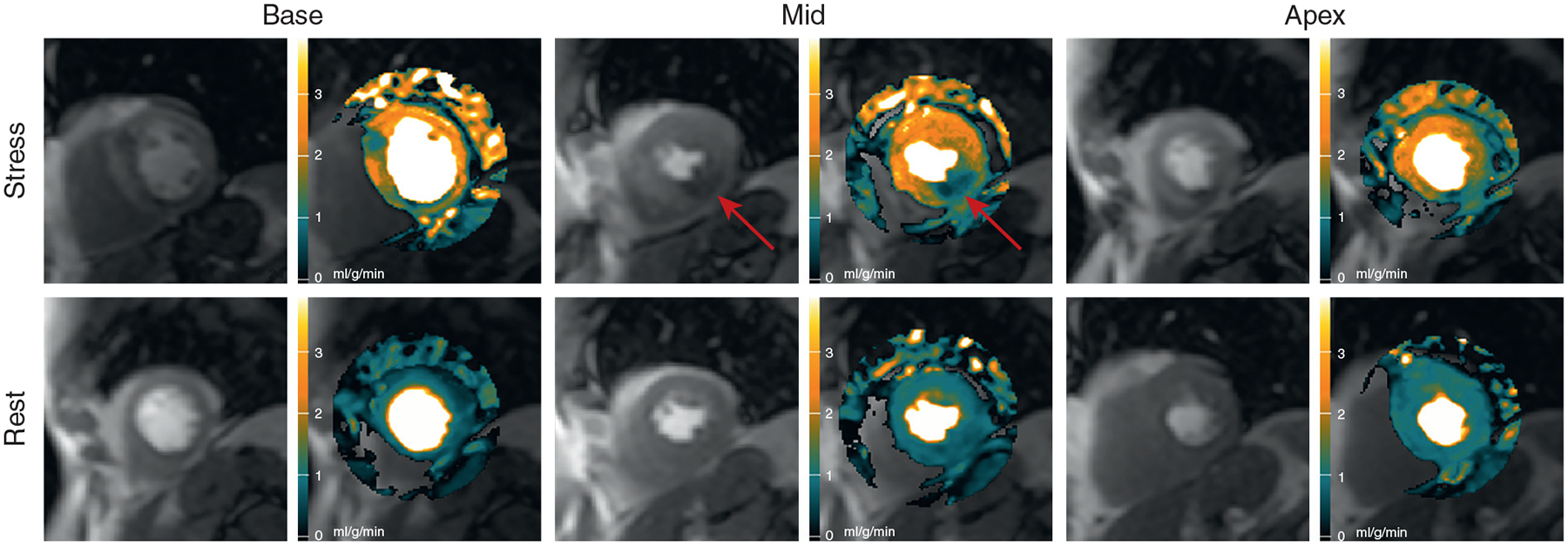
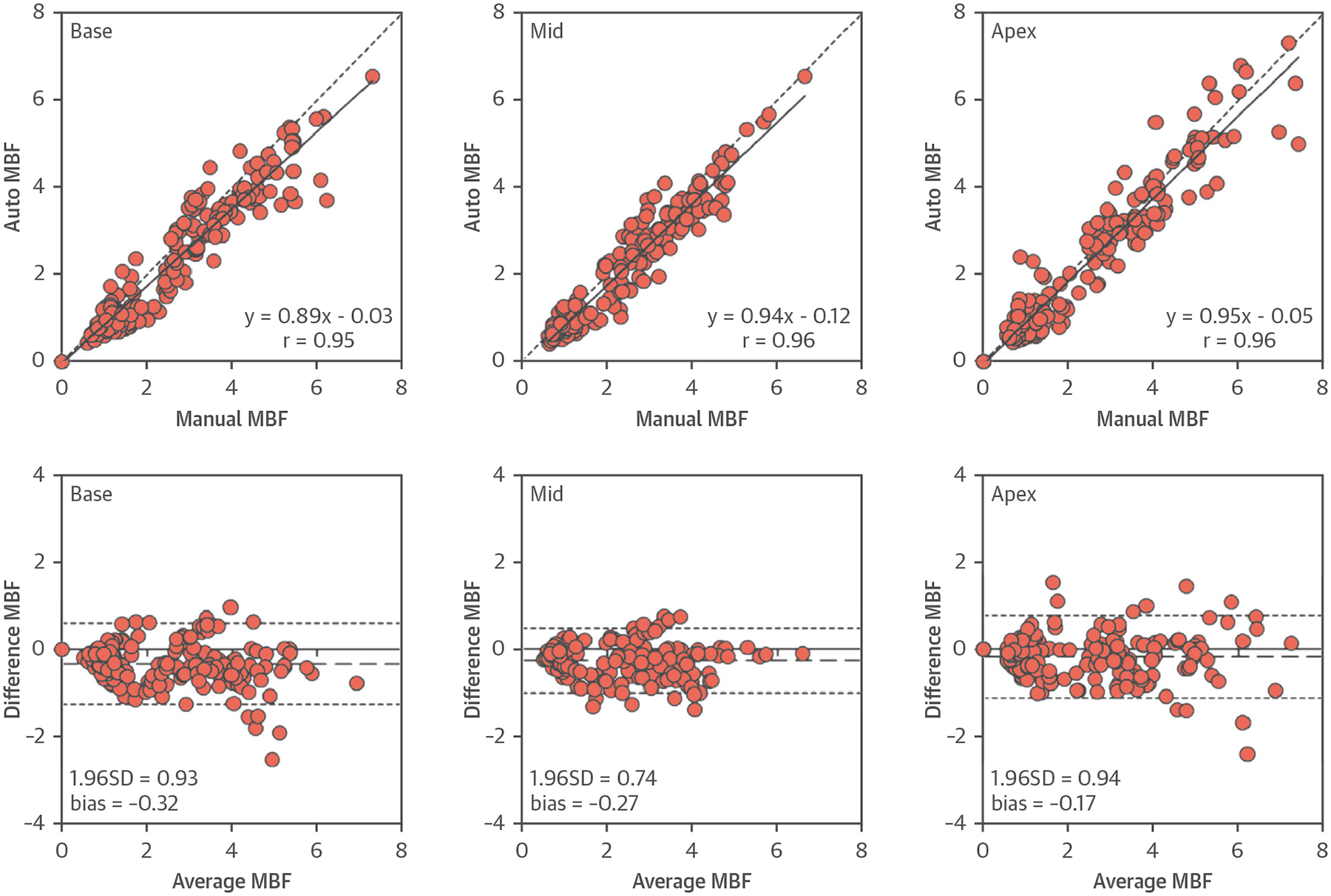
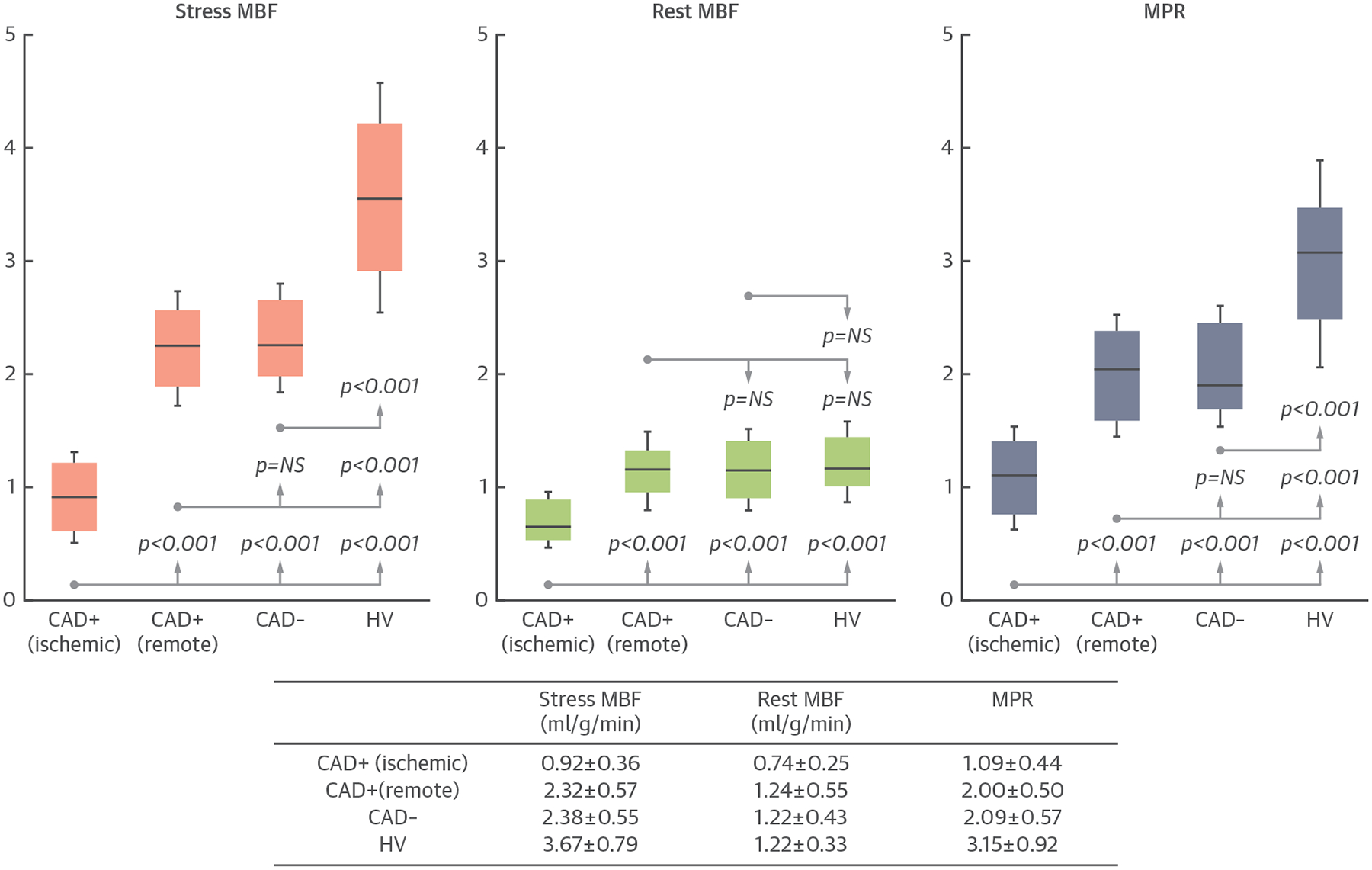
The correlation between automated and manual quantification was excellent (r = 0.96). Stress MBF and MPR in the ischemic zone were lower than those in the remote myocardium in patients with significant CAD (both p < 0.001). Stress MBF and MPR in the remote zone of the patients were lower than those in the normal volunteers (both p < 0.001). All quantitative metrics had good area under the curve (0.864 to 0.926), sensitivity (82.9% to 91.4%), and specificity (75.6% to 91.1%) on per-patient analysis. On a per-vessel analysis of the quantitative metrics, area under the curve (0.837 to 0.864), sensitivity (75.0% to 82.7%), and specificity (71.8% to 80.9%) were good.
Fully quantitative CMR MBF pixel maps can be generated automatically, and the results agree well with manual quantification. These methods can discriminate regional perfusion variations and have high diagnostic performance for detecting significant CAD. (Technical Development of Cardiovascular Magnetic Resonance Imaging; NCT00027170).
作者开发了一种完全自动化的框架,用于从对比增强心脏磁共振(CMR)灌注成像中定量测量心肌血流(MBF),并评估其在患者中的诊断性能。
以前已经通过微球 MBF 测量对完全定量的 CMR 灌注像素图进行了验证,并且显示出了在临床应用中的潜力,但是这些方法需要繁琐的手动过程,并且过于耗时。
对 80 例已知或疑似冠状动脉疾病(CAD)患者和 17 例健康志愿者进行 CMR 灌注成像。定量冠状动脉造影(QCA)定义为≥70%狭窄的 CAD 为显著 CAD;QCA 定义为<70%狭窄或冠状动脉计算机断层血管造影术(CCTA)定义为<30%狭窄且所有血管的钙评分均为 0 的 CAD 为非显著 CAD。与健康志愿者的手动定量相比,自动生成的 MBF 图进行比较。使用绝对 MBF、心肌灌注储备(MPR)和 MBF 和 MPR 的相对测量值,对患者的自动 MBF 像素图的诊断性能进行分析。
自动和手动定量之间的相关性很好(r=0.96)。有显著 CAD 的患者的缺血区的应激 MBF 和 MPR 均低于远隔心肌(均 p<0.001)。患者的远隔区的应激 MBF 和 MPR 均低于正常志愿者(均 p<0.001)。所有定量指标在患者的逐例分析中均具有良好的曲线下面积(0.864 至 0.926)、敏感性(82.9%至 91.4%)和特异性(75.6%至 91.1%)。在定量指标的逐支血管分析中,曲线下面积(0.837 至 0.864)、敏感性(75.0%至 82.7%)和特异性(71.8%至 80.9%)均较好。
完全定量的 CMR MBF 像素图可以自动生成,并且结果与手动定量吻合良好。这些方法可以区分区域性灌注变化,对检测显著 CAD 具有较高的诊断性能。(心血管磁共振成像技术发展;NCT00027170)。