Kellman Peter, Hansen Michael S, Nielles-Vallespin Sonia, Nickander Jannike, Themudo Raquel, Ugander Martin, Xue Hui
National Heart, Lung, and Blood Institute, National Institutes of Health, DHHS, 10 Center Drive MSC-1061, Bethesda, MD, 20892, USA.
Department of Clinical Physiology, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden.
J Cardiovasc Magn Reson. 2017 Apr 7;19(1):43. doi: 10.1186/s12968-017-0355-5.
Quantification of myocardial blood flow requires knowledge of the amount of contrast agent in the myocardial tissue and the arterial input function (AIF) driving the delivery of this contrast agent. Accurate quantification is challenged by the lack of linearity between the measured signal and contrast agent concentration. This work characterizes sources of non-linearity and presents a systematic approach to accurate measurements of contrast agent concentration in both blood and myocardium.
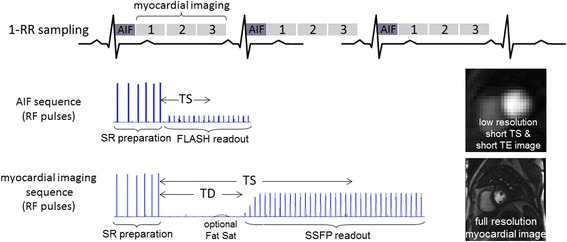
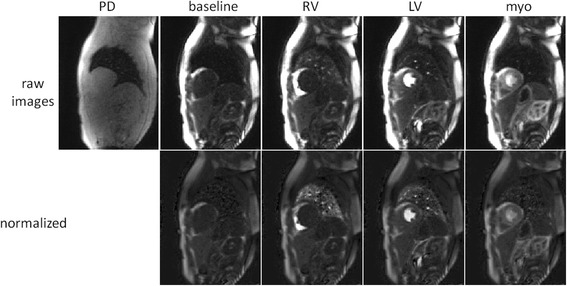
A dual sequence approach with separate pulse sequences for AIF and myocardial tissue allowed separate optimization of parameters for blood and myocardium. A systems approach to the overall design was taken to achieve linearity between signal and contrast agent concentration. Conversion of signal intensity values to contrast agent concentration was achieved through a combination of surface coil sensitivity correction, Bloch simulation based look-up table correction, and in the case of the AIF measurement, correction of T2* losses. Validation of signal correction was performed in phantoms, and values for peak AIF concentration and myocardial flow are provided for 29 normal subjects for rest and adenosine stress.
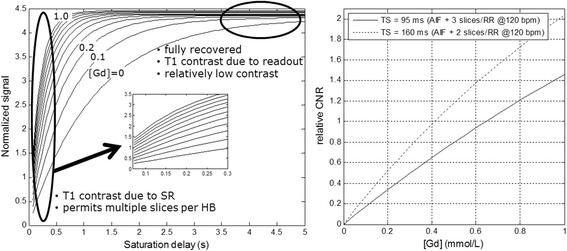
For phantoms, the measured fits were within 5% for both AIF and myocardium. In healthy volunteers the peak [Gd] was 3.5 ± 1.2 for stress and 4.4 ± 1.2 mmol/L for rest. The T2* in the left ventricle blood pool at peak AIF was approximately 10 ms. The peak-to-valley ratio was 5.6 for the raw signal intensities without correction, and was 8.3 for the look-up-table (LUT) corrected AIF which represents approximately 48% correction. Without T2* correction the myocardial blood flow estimates are overestimated by approximately 10%. The signal-to-noise ratio of the myocardial signal at peak enhancement (1.5 T) was 17.7 ± 6.6 at stress and the peak [Gd] was 0.49 ± 0.15 mmol/L. The estimated perfusion flow was 3.9 ± 0.38 and 1.03 ± 0.19 ml/min/g using the BTEX model and 3.4 ± 0.39 and 0.95 ± 0.16 using a Fermi model, for stress and rest, respectively.
A dual sequence for myocardial perfusion cardiovascular magnetic resonance and AIF measurement has been optimized for quantification of myocardial blood flow. A validation in phantoms was performed to confirm that the signal conversion to gadolinium concentration was linear. The proposed sequence was integrated with a fully automatic in-line solution for pixel-wise mapping of myocardial blood flow and evaluated in adenosine stress and rest studies on N = 29 normal healthy subjects. Reliable perfusion mapping was demonstrated and produced estimates with low variability.
心肌血流量的量化需要了解心肌组织中造影剂的量以及驱动这种造影剂输送的动脉输入函数(AIF)。测量信号与造影剂浓度之间缺乏线性关系对准确量化提出了挑战。这项工作描述了非线性的来源,并提出了一种系统方法来准确测量血液和心肌中的造影剂浓度。
采用双序列方法,分别使用用于AIF和心肌组织的脉冲序列,从而可以分别优化血液和心肌的参数。采用系统方法进行整体设计,以实现信号与造影剂浓度之间的线性关系。通过表面线圈灵敏度校正、基于Bloch模拟的查找表校正,以及在AIF测量中校正T2*损失的组合,将信号强度值转换为造影剂浓度。在体模中对信号校正进行了验证,并提供了29名正常受试者静息和腺苷负荷状态下的AIF峰值浓度和心肌血流量值。
对于体模,AIF和心肌的测量拟合误差均在5%以内。在健康志愿者中,负荷状态下的[钆]峰值为3.5±1.2,静息状态下为4.4±1.2 mmol/L。AIF峰值时左心室血池的T2约为10 ms。未校正的原始信号强度的峰谷比为5.6,查找表(LUT)校正后的AIF峰谷比为8.3,代表约48%的校正。未进行T2校正时,心肌血流量估计值高估约10%。负荷状态下心肌信号在峰值增强时(1.5 T)的信噪比为17.7±6.6,[钆]峰值为0.49±0.15 mmol/L。使用BTEX模型,负荷和静息状态下估计的灌注血流量分别为3.9±0.38和1.03±0.19 ml/min/g,使用费米模型时分别为3.4±0.39和0.95±0.16。
用于心肌灌注心血管磁共振和AIF测量的双序列已针对心肌血流量的量化进行了优化。在体模中进行了验证,以确认信号转换为钆浓度是线性的。所提出的序列与用于心肌血流量逐像素映射的全自动在线解决方案集成,并在N = 29名正常健康受试者的腺苷负荷和静息研究中进行了评估。结果表明该序列能可靠地进行灌注映射,且估计值的变异性较低。