Health Research Institute, University of Canberra, Canberra, Australia.
School of Psychiatry University of New South Wales, Academic Department for Old Age Psychiatry, Prince of Wales Hospital, Sydney, Australia.
PLoS One. 2018 Feb 23;13(2):e0193319. doi: 10.1371/journal.pone.0193319. eCollection 2018.
Hospital-acquired complications increase length of stay and contribute to poorer patient outcomes. Older adults are known to be at risk for four key hospital-acquired complications (pressure injuries, pneumonia, urinary tract infections and delirium). These complications have been identified as sensitive to nursing characteristics such as staffing levels and level of education. The cost of these complications compared to the cost of admission severity, dementia, other comorbidities or age has not been established.
To investigate costs associated with nurse-sensitive hospital-acquired complications in an older patient population 157,178 overnight public hospital episodes for all patients over age 50 from one Australian state, 2006/07 were examined. A retrospective cohort study design with linear regression analysis provided modelling of length-of-stay costs. Explanatory variables included patient age, sex, comorbidities, admission severity, dementia status, surgical status and four complications. Extra costs were based on above-average length-of-stay for each patient's Diagnosis Related Group from hospital discharge data.
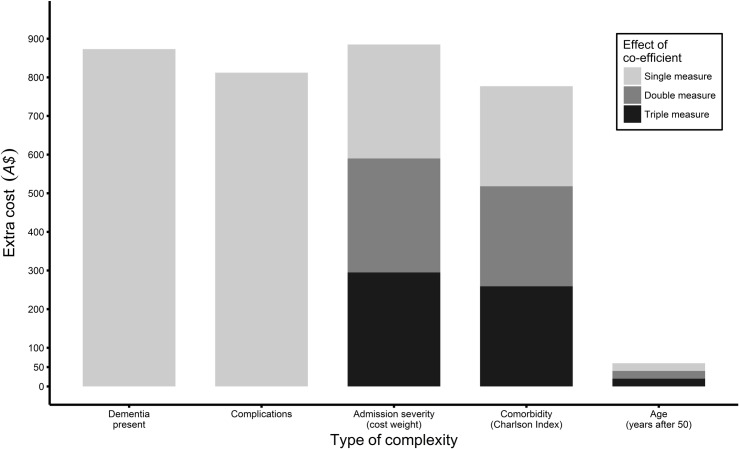
For adults over 50 who have length of stay longer than average for their diagnostic condition, comorbid dementia predicts an extra cost of A$874, (US$1,247); any one of four key complications predicts A$812 (US$1,159); each increase in admission severity score predicts A$295 ($US421); each additional comorbidity predicts A$259 (US$370), and for each year of age above 50 predicts A$20 (US$29) (all estimates significant at p<0.0001).
Hospital-acquired complications and dementia cost more than other kinds of inpatient complexity, but admission severity is a better predictor of excess cost. Because complications are potentially preventable and dementia care in hospitals can be improved, risk-reduction strategies for common complications, particularly for patients with dementia could be cost effective.
Complications and dementia were found to cost more than other kinds of inpatient complexity.
医院获得性并发症会延长住院时间,并导致患者预后较差。老年人已知存在四种关键的医院获得性并发症(压疮、肺炎、尿路感染和谵妄)的风险。这些并发症已被确定对护理特征敏感,如人员配备水平和教育程度。与入院严重程度、痴呆、其他合并症或年龄相比,这些并发症的成本尚未确定。
为了调查澳大利亚一个州所有 50 岁以上患者 157178 例过夜公立医院病例中与老年患者相关的护士敏感型医院获得性并发症的成本,我们对 2006/07 年的数据进行了回顾性队列研究设计,线性回归分析用于建模住院时间成本。解释变量包括患者年龄、性别、合并症、入院严重程度、痴呆状态、手术状态和四种并发症。额外费用基于每位患者从医院出院数据的诊断相关组的平均住院时间。
对于年龄在 50 岁以上、住院时间超过其诊断状况平均时间的成年人,合并痴呆症预计会额外增加 874 澳元(1247 美元)的费用;四种主要并发症中的任何一种都会增加 812 澳元(1159 美元)的费用;入院严重程度评分每增加 1 分,预计会增加 295 澳元(421 美元);每增加一种合并症,预计会增加 259 澳元(370 美元),每增加 1 岁,预计会增加 20 澳元(29 美元)(所有估计均在 p<0.0001 时具有统计学意义)。
医院获得性并发症和痴呆症的成本高于其他类型的住院复杂性,但入院严重程度是超额成本的更好预测指标。由于并发症是潜在可预防的,并且可以改善医院内的痴呆症护理,因此针对常见并发症的风险降低策略,特别是针对痴呆症患者的策略可能具有成本效益。
并发症和痴呆症的成本高于其他类型的住院复杂性。