Adult Critical Care Unit, The Royal London Hospital, Barts Health NHS Trust, Whitechapel Road, London, E1 1BB, UK.
William Harvey Research Institute, Queen Mary University of London, London, UK.
Sci Rep. 2018 Feb 26;8(1):3665. doi: 10.1038/s41598-018-21929-2.
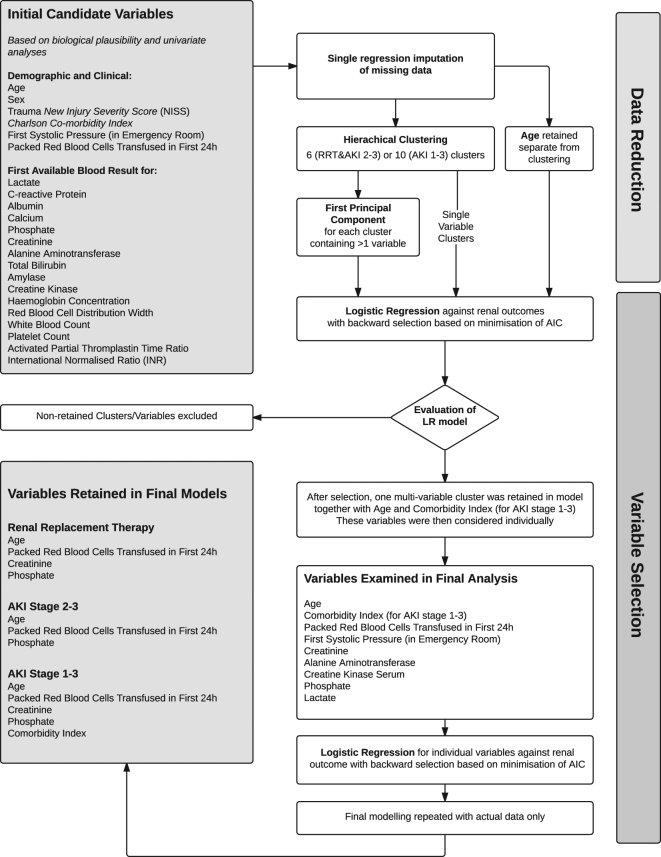
Acute Kidney Injury (AKI) complicating major trauma is associated with increased mortality and morbidity. Traumatic AKI has specific risk factors and predictable time-course facilitating diagnostic modelling. In a single centre, retrospective observational study we developed risk prediction models for AKI after trauma based on data around intensive care admission. Models predicting AKI were developed using data from 830 patients, using data reduction followed by logistic regression, and were independently validated in a further 564 patients. AKI occurred in 163/830 (19.6%) with 42 (5.1%) receiving renal replacement therapy (RRT). First serum creatinine and phosphate, units of blood transfused in first 24 h, age and Charlson score discriminated need for RRT and AKI early after trauma. For RRT c-statistics were good to excellent: development: 0.92 (0.88-0.96), validation: 0.91 (0.86-0.97). Modelling AKI stage 2-3, c-statistics were also good, development: 0.81 (0.75-0.88) and validation: 0.83 (0.74-0.92). The model predicting AKI stage 1-3 performed moderately, development: c-statistic 0.77 (0.72-0.81), validation: 0.70 (0.64-0.77). Despite good discrimination of need for RRT, positive predictive values (PPV) at the optimal cut-off were only 23.0% (13.7-42.7) in development. However, PPV for the alternative endpoint of RRT and/or death improved to 41.2% (34.8-48.1) highlighting death as a clinically relevant endpoint to RRT.
急性肾损伤(AKI)并发于重大创伤与更高的死亡率和发病率相关。创伤性 AKI 具有特定的风险因素和可预测的病程,有利于诊断模型的建立。在一项单中心回顾性观察性研究中,我们根据重症监护室收治情况的数据,建立了创伤后 AKI 的风险预测模型。采用 830 例患者的数据进行 AKI 预测模型的开发,采用数据缩减和逻辑回归,然后在另外 564 例患者中进行独立验证。830 例患者中发生 AKI 163 例(19.6%),42 例(5.1%)接受肾脏替代治疗(RRT)。创伤后早期,首次血清肌酐和磷酸盐、24 小时内输血量、年龄和 Charlson 评分可区分是否需要 RRT 和 AKI。对于 RRT,c 统计值较好到极好:开发:0.92(0.88-0.96),验证:0.91(0.86-0.97)。预测 AKI 2-3 期的模型,c 统计值也较好,开发:0.81(0.75-0.88),验证:0.83(0.74-0.92)。预测 AKI 1-3 期的模型表现中等,开发:c 统计值 0.77(0.72-0.81),验证:0.70(0.64-0.77)。尽管 RRT 需求的区分度较好,但在开发时,最佳切点的阳性预测值(PPV)仅为 23.0%(13.7-42.7)。然而,替代终点(RRT 和/或死亡)的 PPV 提高到 41.2%(34.8-48.1),这突出了死亡作为 RRT 的一个临床相关终点。