Rabello Doralina do Amaral, Ferreira Vivian D'Afonseca da Silva, Berzoti-Coelho Maria Gabriela, Burin Sandra Mara, Magro Cíntia Leticia, Cacemiro Maira da Costa, Simões Belinda Pinto, Saldanha-Araujo Felipe, de Castro Fabíola Attié, Pittella-Silva Fabio
1Laboratory of Molecular Pathology of Cancer, Faculty of Health Sciences and Medicine, University of Brasilia, Brasília, DF Brazil.
2Department of Clinical Analysis, Toxicology and Food Sciences, School of Pharmaceutical Sciences of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP Brazil.
Cancer Cell Int. 2018 Feb 20;18:26. doi: 10.1186/s12935-018-0523-1. eCollection 2018.
Chronic myeloid leukemia (CML) is a clonal myeloproliferative neoplasm whose pathogenesis is linked to the Philadelphia chromosome presence that generates the -1 fusion oncogene. Tyrosine kinase inhibitors (TKI) such as imatinib mesylate (IM) dramatically improved the treatment efficiency and survival of CML patients by targeting BCR-ABL tyrosine kinase. The disease shows three distinct clinical-laboratory stages: chronic phase, accelerated phase and blast crisis. Although patients in the chronic phase respond well to treatment, patients in the accelerated phase or blast crisis usually show therapy resistance and CML relapse. It is crucial, therefore, to identify biomarkers to predict CML genetic evolution and resistance to TKI therapy, considering not only the effects of genetic aberrations but also the role of epigenetic alterations during the disease. Although dysregulations in epigenetic modulators such as histone methyltrasnferases have already been described for some hematologic malignancies, to date very limited data is available for CML, especially when considering the lysine methyltransferase and .
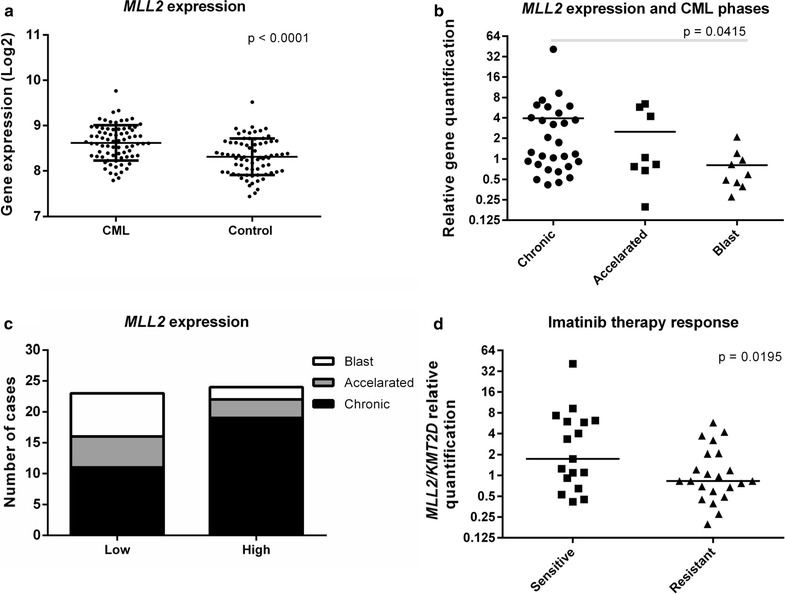
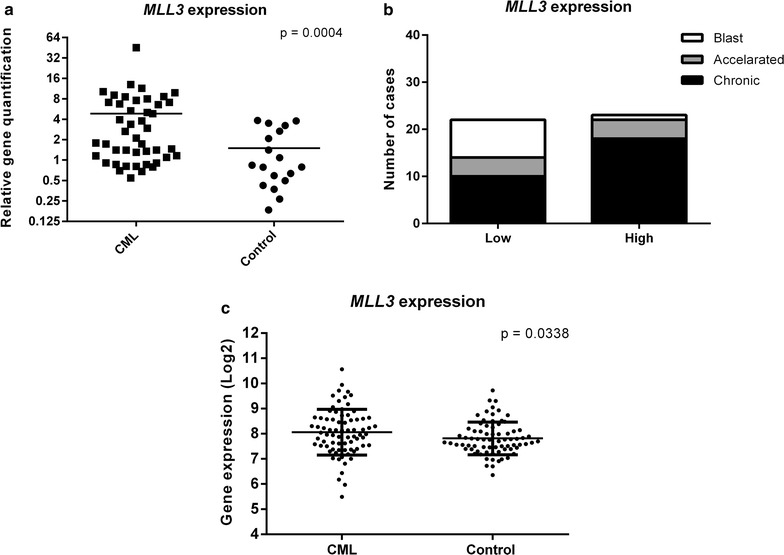
Here we investigated the expression profile of both genes in CML patients in different stages of the disease, in patients showing different responses to therapy with IM and in non-neoplastic control samples. Imatinib sensitive and resistant CML cell lines were also used to investigate whether treatment with other tyrosine kinase inhibitors interfered in their expression.
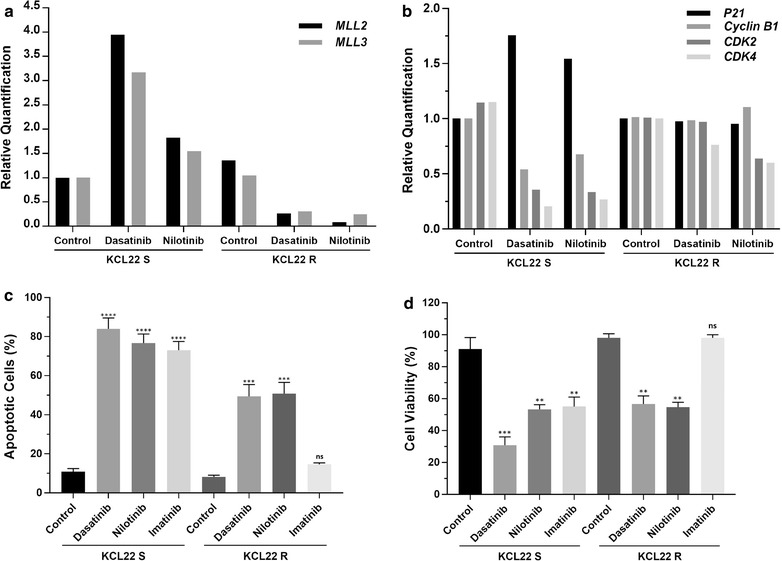
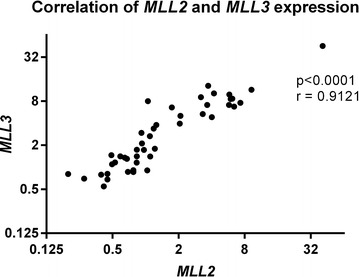
In patients, both methyltransferases were either upregulated or with basal expression level during the chronic phase compared to controls. Interestingly, and specially levels decreased during disease progression correlating with distinct clinical stages. Furthermore, was decreased in patients resistant to IM treatment. A rescue in the expression of both genes was observed in KCL22S, a CML cell line sensitive to IM, after treatment with dasatinib or nilotinib which was associated with a higher rate of apoptosis, an enhanced expression of () and a concomitant decrease in the expression of , and in comparison to untreated KCL22S control or IM resistant KCL22R cell line, which suggests involvement of p53 regulated pathway.
Our results established a new association between and genes with CML and suggest that is associated with disease evolution and may be a potential marker to predict the development of therapy resistance.
慢性髓性白血病(CML)是一种克隆性骨髓增殖性肿瘤,其发病机制与产生BCR-ABL1融合致癌基因的费城染色体的存在有关。酪氨酸激酶抑制剂(TKI),如甲磺酸伊马替尼(IM),通过靶向BCR-ABL酪氨酸激酶显著提高了CML患者的治疗效果和生存率。该疾病表现出三个不同的临床-实验室阶段:慢性期、加速期和急变期。尽管慢性期患者对治疗反应良好,但加速期或急变期患者通常表现出治疗抵抗和CML复发。因此,考虑到不仅遗传畸变的影响,而且疾病过程中表观遗传改变的作用,识别预测CML基因演变和对TKI治疗抵抗的生物标志物至关重要。尽管表观遗传调节剂如组蛋白甲基转移酶的失调已在一些血液系统恶性肿瘤中有所描述,但迄今为止,关于CML的数据非常有限,尤其是考虑赖氨酸甲基转移酶SETD2和KMT2D时。
在这里,我们研究了这两个基因在疾病不同阶段的CML患者、对IM治疗表现出不同反应的患者以及非肿瘤对照样本中的表达谱。伊马替尼敏感和耐药的CML细胞系也用于研究用其他酪氨酸激酶抑制剂治疗是否会干扰它们的表达。
在患者中,与对照组相比,慢性期两种甲基转移酶均上调或处于基础表达水平。有趣的是,随着疾病进展,SETD2和特别是KMT2D水平下降,这与不同的临床阶段相关。此外,IM治疗耐药的患者中KMT2D降低。在用达沙替尼或尼洛替尼治疗后,在对IM敏感的CML细胞系KCL22S中观察到这两个基因的表达恢复,这与更高的凋亡率、p21(CDKN1A)表达增强以及与未处理的KCL22S对照或IM耐药的KCL22R细胞系相比,p53、MDM2和MCL1表达的同时降低有关,这表明p53调节通路的参与。
我们的结果建立了SETD2和KMT2D基因与CML之间的新关联,并表明KMT2D与疾病演变相关,可能是预测治疗抵抗发展的潜在标志物。