Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Primary Care Unit, Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK.
Lancet. 2018 Mar 10;391(10124):949-959. doi: 10.1016/S0140-6736(18)30309-X. Epub 2018 Feb 27.
Studies evaluating titration of antihypertensive medication using self-monitoring give contradictory findings and the precise place of telemonitoring over self-monitoring alone is unclear. The TASMINH4 trial aimed to assess the efficacy of self-monitored blood pressure, with or without telemonitoring, for antihypertensive titration in primary care, compared with usual care.
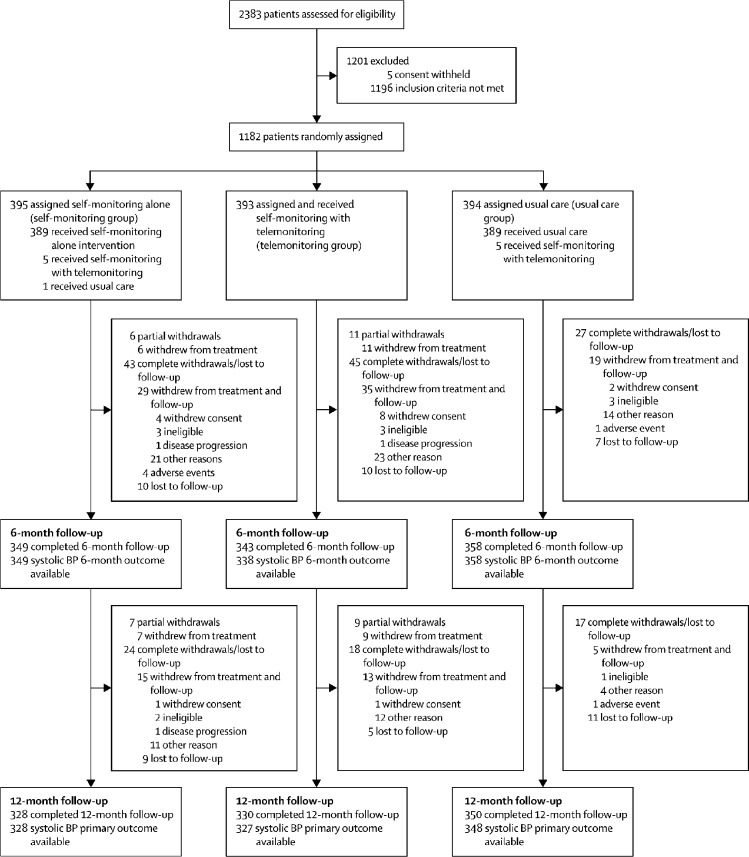
This study was a parallel randomised controlled trial done in 142 general practices in the UK, and included hypertensive patients older than 35 years, with blood pressure higher than 140/90 mm Hg, who were willing to self-monitor their blood pressure. Patients were randomly assigned (1:1:1) to self-monitoring blood pressure (self-montoring group), to self-monitoring blood pressure with telemonitoring (telemonitoring group), or to usual care (clinic blood pressure; usual care group). Randomisation was by a secure web-based system. Neither participants nor investigators were masked to group assignment. The primary outcome was clinic measured systolic blood pressure at 12 months from randomisation. Primary analysis was of available cases. The trial is registered with ISRCTN, number ISRCTN 83571366.
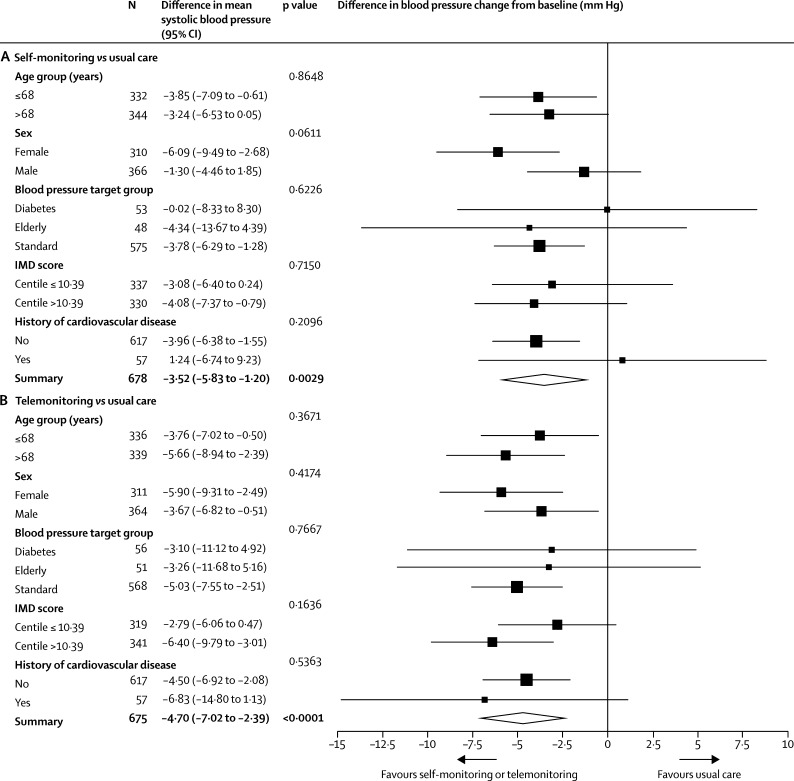
1182 participants were randomly assigned to the self-monitoring group (n=395), the telemonitoring group (n=393), or the usual care group (n=394), of whom 1003 (85%) were included in the primary analysis. After 12 months, systolic blood pressure was lower in both intervention groups compared with usual care (self-monitoring, 137·0 [SD 16·7] mm Hg and telemonitoring, 136·0 [16·1] mm Hg vs usual care, 140·4 [16·5]; adjusted mean differences vs usual care: self-monitoring alone, -3·5 mm Hg [95% CI -5·8 to -1·2]; telemonitoring, -4·7 mm Hg [-7·0 to -2·4]). No difference between the self-monitoring and telemonitoring groups was recorded (adjusted mean difference -1·2 mm Hg [95% CI -3·5 to 1·2]). Results were similar in sensitivity analyses including multiple imputation. Adverse events were similar between all three groups.
Self-monitoring, with or without telemonitoring, when used by general practitioners to titrate antihypertensive medication in individuals with poorly controlled blood pressure, leads to significantly lower blood pressure than titration guided by clinic readings. With most general practitioners and many patients using self-monitoring, it could become the cornerstone of hypertension management in primary care.
National Institute for Health Research via Programme Grant for Applied Health Research (RP-PG-1209-10051), Professorship to RJM (NIHR-RP-R2-12-015), Oxford Collaboration for Leadership in Applied Health Research and Care, and Omron Healthcare UK.
使用自我监测来评估降压药物滴定的研究得出了相互矛盾的结果,远程监测相对于单独自我监测的确切作用尚不清楚。TASMINH4 试验旨在评估自我监测血压(伴或不伴远程监测)在初级保健中用于降压滴定的疗效,与常规护理相比。
这是一项在英国 142 家普通诊所进行的平行随机对照试验,纳入了年龄大于 35 岁、血压高于 140/90mmHg、愿意自我监测血压的高血压患者。患者被随机分配(1:1:1)接受自我监测血压(自我监测组)、自我监测血压加远程监测(远程监测组)或常规护理(诊所血压;常规护理组)。随机分配通过安全的基于网络的系统进行。参与者和研究人员均未对分组分配情况进行设盲。主要结局为随机分组后 12 个月时诊所测量的收缩压。主要分析为可用病例分析。该试验在 ISRCTN 注册,编号 ISRCTN 83571366。
1182 名参与者被随机分配至自我监测组(n=395)、远程监测组(n=393)或常规护理组(n=394),其中 1003 名(85%)纳入主要分析。12 个月后,与常规护理相比,两组干预组的收缩压均较低(自我监测组为 137.0[16.7]mmHg,远程监测组为 136.0[16.1]mmHg,常规护理组为 140.4[16.5]mmHg;与常规护理相比的调整平均差异:自我监测单独治疗组为-3.5mmHg[95%CI-5.8 至-1.2];远程监测组为-4.7mmHg[-7.0 至-2.4])。自我监测组和远程监测组之间未记录到差异(调整平均差异-1.2mmHg[95%CI-3.5 至 1.2])。包括多重插补的敏感性分析结果相似。所有三组的不良事件相似。
由全科医生使用自我监测(伴或不伴远程监测)来调整血压控制不佳的个体的降压药物剂量,可显著降低血压,优于根据诊所读数进行调整。随着大多数全科医生和许多患者使用自我监测,它可能成为初级保健中高血压管理的基石。
英国国民健康保险制度通过应用健康研究计划拨款(RP-PG-1209-10051)、为 RJM 教授职位(NIHR-RP-R2-12-015)、牛津应用健康研究和护理合作组织以及欧姆龙医疗保健英国提供资金。