Virvidaki Ioanna Eleni, Nasios Grigorios, Kosmidou Maria, Giannopoulos Sotirios, Milionis Haralampos
Department of Internal Medicine, School of Medicine, University of Ioannina, Ioannina, Greece.
Department of Speech and Language Therapy, Technological Educational Institute of Epirus, Ioannina, Greece.
J Clin Neurol. 2018 Jul;14(3):265-274. doi: 10.3988/jcn.2018.14.3.265. Epub 2018 Feb 28.
The presence of dysphagia and aspiration in stroke patients is associated with increased mortality and morbidity. Early recognition and management of these two conditions via reliable, minimally invasive bedside procedures before complications arise remains challenging in everyday clinical practice. This study reviews the available bedside screening tools for detecting swallowing status and aspiration risk in acute stroke by qualitatively observing reference population study design, clinical flexibility, reliability and applicability to acute-care settings.
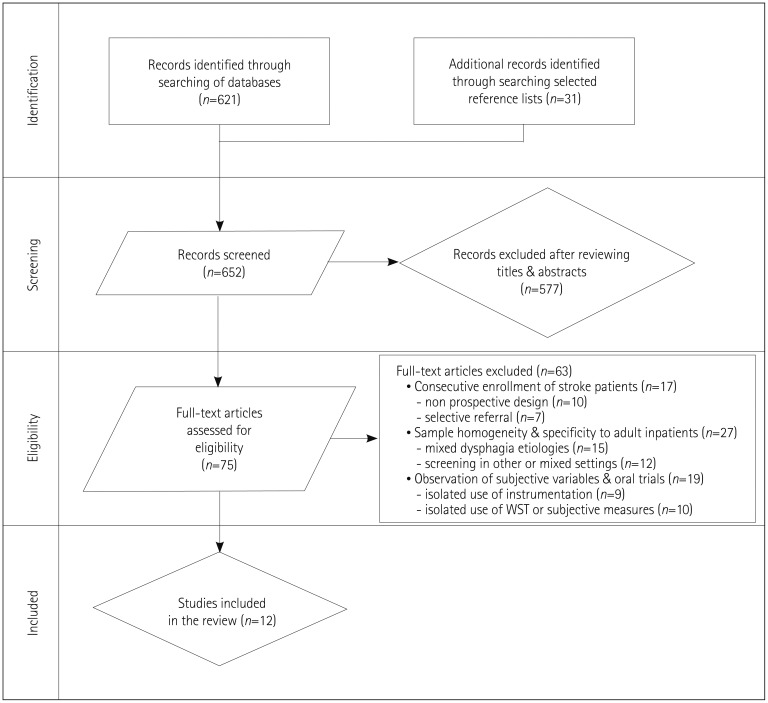
The primary search was conducted using the PubMed, Embase, and Cochrane Library databases. The search was limited to papers on humans written in English and published from 1991 to 2016. Eligibility criteria included the consecutive enrollment of acute-stroke inpatients and the development of a protocol for screening aspiration risk during oral feeding in this population.
Of the 652 sources identified, 75 articles were reviewed in full however, only 12 fulfilled the selection criteria. Notable deficiencies in most of the bedside screening protocols included poor methodological designs and inadequate predictive values for aspiration risk which render clinicians to be more conservative in making dietary recommendations.
The literature is dense with screening methods for assessing the presence of dysphagia but with low predictive value for aspiration risk after acute stroke. A standard, practical, and cost-effective screening tool that can be applied at the bedside and interpreted by a wide range of hospital personnel remains to be developed. This need is highlighted in settings where neither trained personnel in evaluating dysphagia nor clinical instrumentation procedures are available.
中风患者吞咽困难和误吸的存在与死亡率和发病率的增加相关。在日常临床实践中,在并发症出现之前通过可靠的、微创的床边程序对这两种情况进行早期识别和管理仍然具有挑战性。本研究通过定性观察参考人群研究设计、临床灵活性、可靠性以及对急性护理环境的适用性,回顾了现有的用于检测急性中风患者吞咽状态和误吸风险的床边筛查工具。
主要检索使用了PubMed、Embase和Cochrane图书馆数据库。检索限于1991年至2016年发表的英文撰写的关于人类的论文。纳入标准包括连续纳入急性中风住院患者以及制定该人群经口进食期间筛查误吸风险的方案。
在识别出的652篇文献中,对75篇文章进行了全文回顾,然而,只有12篇符合选择标准。大多数床边筛查方案的显著不足包括方法学设计不佳以及误吸风险的预测价值不足,这使得临床医生在做出饮食建议时更加保守。
文献中有大量评估吞咽困难存在的筛查方法,但对急性中风后误吸风险的预测价值较低。仍有待开发一种可在床边应用且能被广泛的医院工作人员解读的标准、实用且经济高效的筛查工具。在既没有受过评估吞咽困难培训的人员也没有临床检测程序的环境中,这种需求尤为突出。