Wiles Jonathan D, Taylor Katrina, Coleman Damian, Sharma Rajan, O'Driscoll Jamie M
Section of Sport & Exercise Sciences, School of Human and Life Sciences, Canterbury Christ Church University Department of Cardiology, St George's Healthcare NHS Trust, London, UK.
Medicine (Baltimore). 2018 Mar;97(10):e0105. doi: 10.1097/MD.0000000000010105.
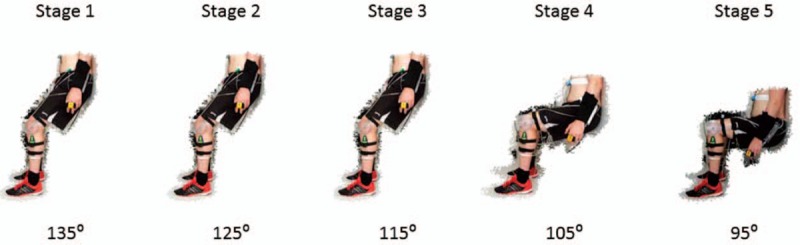
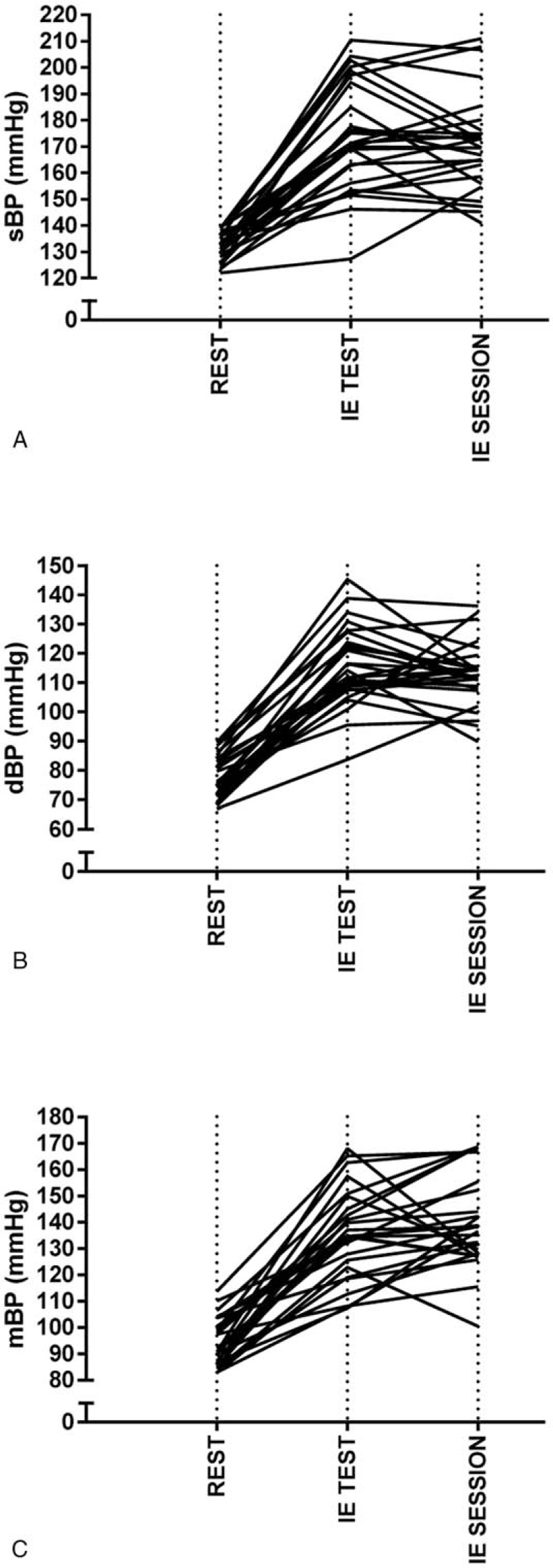
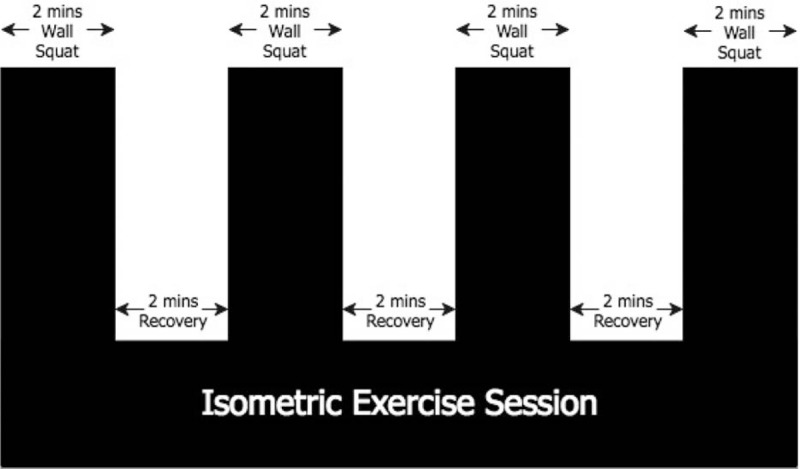
Few studies have investigated the relative safety of prescribing isometric exercise (IE) to reduce resting blood pressure (BP). This study aimed to ascertain the safety of the hemodynamic response during an IE wall squat protocol.Twenty-six hypertensive (BP of 120-139 mm Hg systolic and/or 80-90 mm Hg diastolic) males (45 ± 8 years; 1.78 ± 0.07 m; 89.7 ± 12.3 kg; mean ± SD), visited the laboratory on 2 separate occasions. Heart rate (HR) and BP were measured at rest and continuously throughout exercise. In visit 1, participants completed a continuous incremental isometric wall squat exercise test, starting at 135° of knee flexion, decreasing by 10° every 2 minutes until 95° (final stage). Exercise was terminated upon completion of the test or volitional fatigue. The relationship between knee joint angle and mean HR was used to calculate the participant-specific knee joint angle required to elicit a target HR of 95% HRpeak. This angle was used to determine exercise intensity for a wall squat training session consisting of 4 × 2 minute bouts (visit 2).Systolic BPs during the exercise test and training were 173 ± 21 mm Hg and 171 ± 19 mm Hg, respectively, (P > .05) and were positively related (r = 0.73, P < .05) with ratio limits of agreement (LoA) of 0.995 ×/÷ 1.077. Diastolic BPs were 116 ± 14 mm Hg and 113 ± 11 mm Hg, respectively, (P > .05) and were positively related (r = 0.42, P < .05) with ratio LoA of 0.99 ×/÷ 1.107. No participant recorded a systolic BP > 250 mm Hg. Diastolic BP values > 115 mm Hg were recorded in 12 participants during the incremental test and 6 participants during the training session. Peak rate pressure product was 20681 ± 3911 mm Hg bpm during the IE test and was lower (18074 ± 3209 mm Hg bpm) during the IE session (P = .002). No adverse effects were reported.Based on the current ACSM guidelines for aerobic exercise termination, systolic BP does not reach the upper limit during IE in this population. Diastolic BP exceeds 115 mm Hg in some during the IE protocol, which may suggest the need to individualise IE training prescription in some with suboptimal BP control. Future research is required to ascertain if IE requires modified BP termination guidelines.
很少有研究调查开具等长运动(IE)处方以降低静息血压(BP)的相对安全性。本研究旨在确定在IE靠墙深蹲方案期间血流动力学反应的安全性。26名高血压男性(收缩压120 - 139 mmHg和/或舒张压80 - 90 mmHg)(45±8岁;身高1.78±0.07 m;体重89.7±12.3 kg;均值±标准差)分两次到实验室就诊。在静息状态下以及运动全程连续测量心率(HR)和血压。在第一次就诊时,参与者完成连续递增的靠墙深蹲运动测试,从膝关节屈曲135°开始,每2分钟减少10°直至95°(最后阶段)。测试完成或出现自愿性疲劳时终止运动。利用膝关节角度与平均心率之间的关系计算出引发95%心率峰值所需的个体特异性膝关节角度。该角度用于确定由4组每组2分钟的靠墙深蹲训练课(第二次就诊)的运动强度。运动测试和训练期间的收缩压分别为173±21 mmHg和171±19 mmHg,(P>0.05),且呈正相关(r = 0.73,P<0.05),一致性界限(LoA)为0.995×/÷1.077。舒张压分别为116±14 mmHg和113±11 mmHg,(P>0.05),且呈正相关(r = 0.42,P<0.05),比率LoA为0.99×/÷1.107。没有参与者记录到收缩压>250 mmHg。在递增测试期间12名参与者以及训练期间6名参与者记录到舒张压值>115 mmHg。等长运动测试期间的峰值速率压力乘积为20681±3911 mmHg·bpm,等长运动课期间较低(18074±3209 mmHg·bpm)(P = 0.002)。未报告不良反应。根据美国运动医学学会当前关于有氧运动终止的指南,该人群在进行等长运动期间收缩压未达到上限。在等长运动方案期间,部分人的舒张压超过115 mmHg,这可能表明对于血压控制欠佳的部分人需要个体化等长运动训练处方。需要进一步研究以确定等长运动是否需要修改血压终止指南。