Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota.
Division of Gastroenterology and Hepatology, Carilion Clinic, Roanoke, Virginia.
Inflamm Bowel Dis. 2018 Apr 23;24(5):1074-1081. doi: 10.1093/ibd/izx096.
The course of inflammatory bowel disease (IBD) after liver transplantation (LT) for primary sclerosing cholangitis (PSC) is poorly understood. We describe the natural history of established IBD after LT (including risk of disease progression, colectomy, and neoplasia) and de novo IBD.
In a retrospective cohort, we identified all patients with PSC who underwent LT for advanced PSC at Mayo Clinic, Rochester, Minnesota. Risk factors were identified using multivariate Cox proportional hazard analysis.
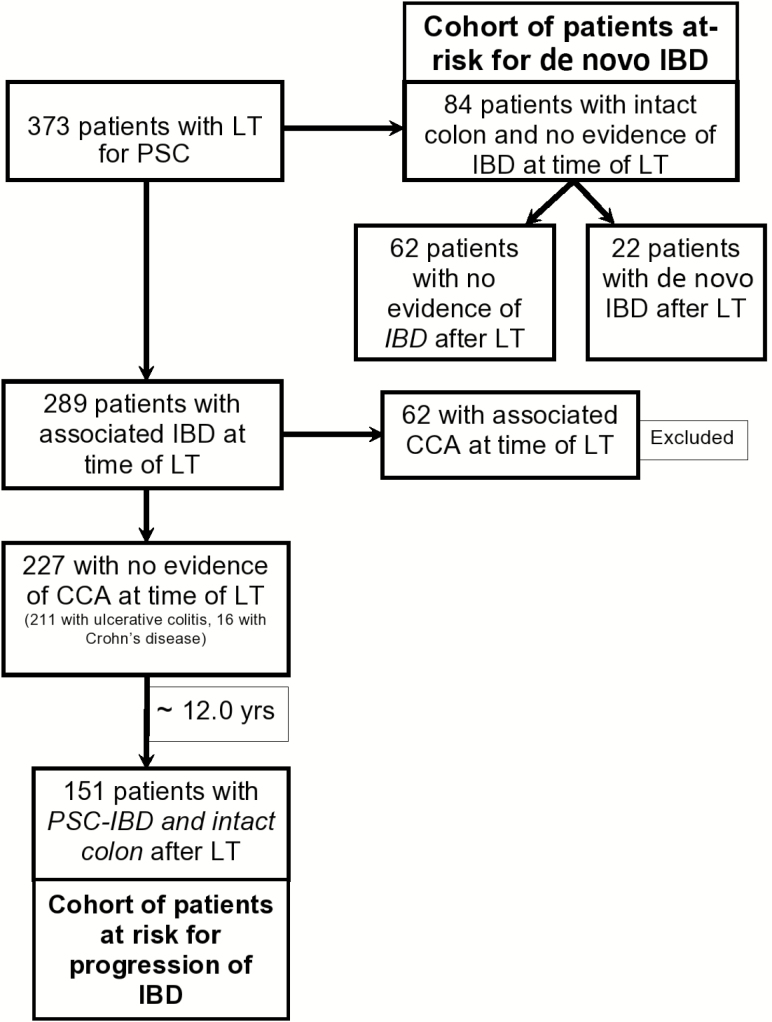
Three hundred seventy-three patients were identified (mean age, 47.5 ± 11.7 years; 64.9% male). Over a median (range) of 10 (5.5-17.1) years, 151 patients with PSC-IBD with an intact colon at the time of LT were studied. Post-LT, despite transplant-related immunosuppression, 56/151 (37.1%) required escalation of therapy, whereas 87 had a stable course (57.6%) and 8 patients (5.3%) improved. The 1-, 5-, and 10-year risks of progression of IBD were 4.0%, 18.5%, and 25.5%, respectively. On multivariate analysis, tacrolimus-based immunosuppression post-LT were associated with unfavorable course, and azathioprine use after LT was associated with improved course post-LT. Of 84 patients with no evidence of IBD at the time of LT, 22 (26.2%) developed de novo IBD post-LT. The 1-, 5-, and 10-year cumulative incidences of de novo IBD were 5.5%, 20.0%, and 25.4%, respectively. On univariate analysis, mycophenolate mofetil use after LT was associated with increased risk of de novo IBD, but azathioprine use after LT seemed to be protective.
The 10-year cumulative probability of IBD flare requiring escalation of therapy after LT for PSC was 25.5%, despite immunosuppression for LT. The 10-year cumulative risk of de novo IBD after LT for PSC was 25.4%. Transplant-related immunosuppression may modify the risk of de novo IBD, with an increased risk with mycophenolate and a decreased risk with azathioprine. 10.1093/ibd/izx096_video1izx096.video15746673864001.
原发性硬化性胆管炎(PSC)患者行肝移植(LT)后炎症性肠病(IBD)的病程尚不清楚。我们描述了 LT 后已确诊 IBD(包括疾病进展、结肠切除术和肿瘤发生的风险)和新发 IBD 的自然病程。
在一项回顾性队列研究中,我们确定了明尼苏达州罗切斯特市梅奥诊所所有因晚期 PSC 而行 LT 的 PSC 患者。采用多变量 Cox 比例风险分析确定危险因素。
共确定了 373 例患者(平均年龄 47.5 ± 11.7 岁;64.9%为男性)。在中位(范围)10(5.5-17.1)年的随访中,研究了 151 例 LT 时结肠完整的 PSC-IBD 患者。尽管存在移植相关免疫抑制,但 LT 后仍有 56/151(37.1%)需要升级治疗,87 例病情稳定(57.6%),8 例(5.3%)有所改善。IBD 进展的 1、5 和 10 年风险分别为 4.0%、18.5%和 25.5%。多变量分析显示,LT 后使用他克莫司为基础的免疫抑制剂与不良病程相关,LT 后使用巯嘌呤与 LT 后病情改善相关。84 例 LT 时无 IBD 证据的患者中,22 例(26.2%)在 LT 后新发 IBD。LT 后新发 IBD 的 1、5 和 10 年累积发生率分别为 5.5%、20.0%和 25.4%。单变量分析显示,LT 后使用霉酚酸酯与新发 IBD 的风险增加相关,但 LT 后使用巯嘌呤似乎有保护作用。
尽管 LT 用于治疗 PSC,但 PSC 患者 LT 后 IBD 发作需要升级治疗的 10 年累积概率为 25.5%。PSC 患者 LT 后新发 IBD 的 10 年累积风险为 25.4%。移植相关免疫抑制可能改变新发 IBD 的风险,霉酚酸酯的风险增加,巯嘌呤的风险降低。