Matharu Gulraj S, Judge Andrew, Murray David W, Pandit Hemant G
G. S. Matharu, A. Judge, D. W. Murray, H. G. Pandit, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Nuffield Orthopaedic Centre, Oxford, UK A. Judge, MRC Lifecourse Epidemiology Unit, Southampton General Hospital, University of Southampton, Southampton, UK H. G. Pandit, Leeds Institute of Rheumatic and Musculoskeletal Medicine, Chapel Allerton Hospital, Leeds, UK.
Clin Orthop Relat Res. 2018 Feb;476(2):245-258. doi: 10.1007/s11999.0000000000000029.
Metal-on-metal hip replacement (MoMHR) revision surgery for adverse reactions to metal debris (ARMD) has been associated with an increased risk of early complications and reoperation and inferior patient-reported outcome scores compared with non-ARMD revisions. As a result, early revision specifically for ARMD with adoption of a lower surgical threshold has been widely recommended with the goal of improving the subsequent prognosis after ARMD revisions. However, no large cohorts have compared the risk of complications and reoperation after MoMHR revision surgery for ARMD (an unanticipated revision indication) with those after non-ARMD revisions (which represent conventional modes of arthroplasty revision).
QUESTIONS/PURPOSES: (1) Does the risk of intraoperative complications differ between MoMHRs revised for ARMD compared with non-ARMD indications? (2) Do mortality rates differ after MoMHRs revised for ARMD compared with non-ARMD indications? (3) Do rerevision rates differ after MoMHRs revised for ARMD compared with non-ARMD indications? (4) How do implant survival rates differ after MoMHR revision when performed for specific non-ARMD indications compared with ARMD?
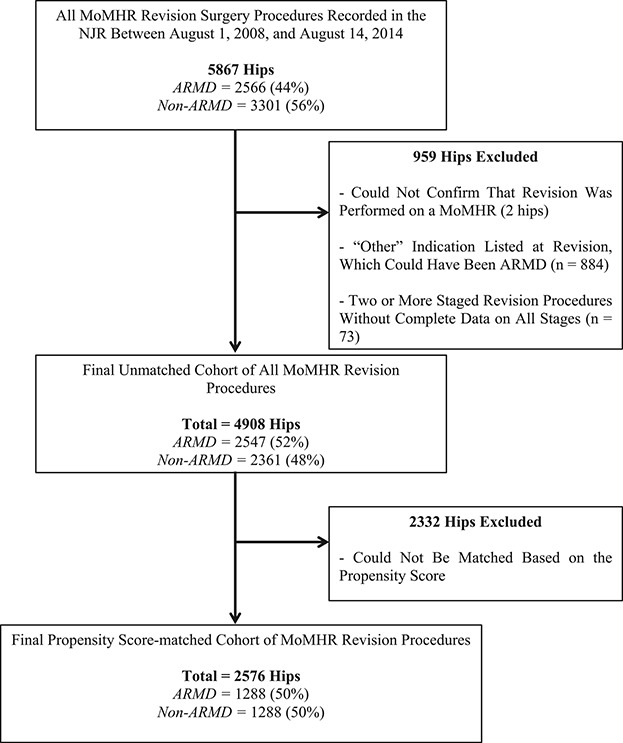
This retrospective observational study involved all patients undergoing MoMHR from the National Joint Registry (NJR) for England and Wales subsequently revised for any indication between 2008 and 2014. The NJR achieves high levels of patient consent (93%) and linked procedures (ability to link serial procedures performed on the same patient and hip; 95%). Furthermore, recent validation studies have demonstrated that when revision procedures have been captured within the NJR, the data completion and accuracy were excellent. Revisions for ARMD and non-ARMD indications were matched one to one for multiple potential confounding factors using propensity scores. The propensity score summarizes the many patient and surgical factors that were used in the matching process (including sex, age, type of primary arthroplasty, time to revision surgery, and details about the revision procedure performed such as the approach, specific components revised, femoral head size, bearing surface, and use of bone graft) using one single score for each revised hip. The patient and surgical factors within the ARMD and non-ARMD groups subsequently became much more balanced once the groups had been matched based on the propensity scores. The matched cohort included 2576 MoMHR revisions with each study group including 1288 revisions (mean followup of 3 years for both groups; range, 1-7 years). Intraoperative complications, mortality, and rerevision surgery were compared between matched groups using univariable regression analyses. Implant survival rates in the non-ARMD group were calculated for each specific revision indication with each individual non-ARMD indication subsequently compared with the implant survival rate in the ARMD group using Cox regression analyses.
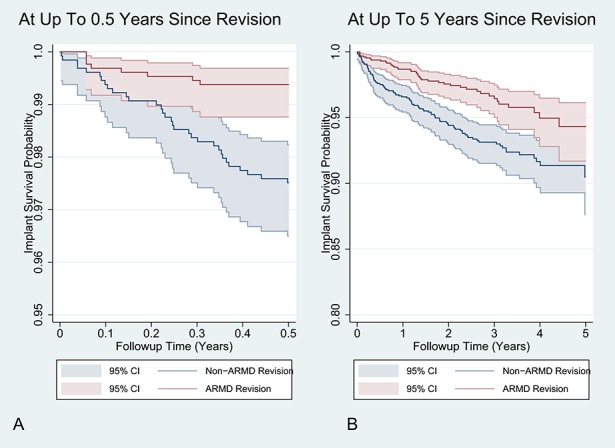
There was no difference between the ARMD and non-ARMD MoMHR revisions in terms of intraoperative complications (odds ratio, 0.97; 95% confidence interval [CI], 0.59-1.59; p = 0.900). Mortality rates were lower after ARMD revision compared with non-ARMD revision (hazard ratio [HR], 0.43; CI, 0.21-0.87; p = 0.019); however, there was no difference when revisions performed for infection were excluded from the non-ARMD indication group (HR, 0.69; CI, 0.35-1.37; p = 0.287). Rerevision rates were lower after ARMD revision compared with non-ARMD revision (HR, 0.52; CI, 0.36-0.75; p < 0.001); this difference persisted even after removing revisions performed for infection (HR, 0.59; CI, 0.40-0.89; p = 0.011). Revisions for infection (5-year survivorship = 81%; CI, 55%-93%; p = 0.003) and dislocation/subluxation (5-year survivorship = 82%; CI, 69%-90%; p < 0.001) had the lowest implant survival rates when compared with revisions for ARMD (5-year survivorship = 94%; CI, 92%-96%).
Contrary to previous observations, MoMHRs revised for ARMD have approximately half the risk of rerevision compared with non-ARMD revisions. We suspect worldwide regulatory authorities have positively influenced rerevision rates after ARMD revision by recommending that surgeons exercise a lower revision threshold and that such revisions are now being performed at an earlier stage. The high risk of rerevision after MoMHR revision for infection and dislocation is concerning. Infected MoMHR revisions were responsible for the increased mortality risk observed after non-ARMD revision, which parallels findings in non-MoMHR revisions for infection.
Level III, therapeutic study.
金属对金属髋关节置换术(MoMHR)因金属碎屑不良反应(ARMD)进行翻修手术,与早期并发症、再次手术风险增加相关,且患者报告的结果评分低于非ARMD翻修手术。因此,为改善ARMD翻修术后的预后,广泛推荐针对ARMD采用较低手术阈值进行早期翻修。然而,尚无大型队列研究比较因ARMD(一种意外的翻修指征)进行MoMHR翻修手术后与非ARMD翻修手术(代表传统关节成形术翻修模式)后的并发症和再次手术风险。
问题/目的:(1)因ARMD进行MoMHR翻修与因非ARMD指征进行MoMHR翻修相比,术中并发症风险是否不同?(2)因ARMD进行MoMHR翻修与因非ARMD指征进行MoMHR翻修相比,死亡率是否不同?(3)因ARMD进行MoMHR翻修与因非ARMD指征进行MoMHR翻修相比,再次翻修率是否不同?(4)针对特定非ARMD指征进行MoMHR翻修与针对ARMD进行MoMHR翻修相比,植入物生存率如何不同?
这项回顾性观察性研究纳入了2008年至2014年间在英格兰和威尔士国家关节注册中心(NJR)接受MoMHR且随后因任何指征进行翻修的所有患者。NJR实现了高水平的患者同意率(93%)和关联程序(能够关联同一患者同一髋关节上进行的系列程序;95%)。此外,近期的验证研究表明,当翻修程序被纳入NJR时,数据完整性和准确性极佳。使用倾向评分将ARMD和非ARMD指征的翻修手术在多个潜在混杂因素上进行一对一匹配。倾向评分汇总了匹配过程中使用的许多患者和手术因素(包括性别、年龄、初次关节成形术类型、翻修手术时间以及所进行翻修手术的详细信息,如手术入路、翻修的特定组件、股骨头大小、关节面以及骨移植的使用情况),每个翻修髋关节使用一个单一分数。基于倾向评分进行匹配后,ARMD组和非ARMD组内的患者和手术因素随后变得更加均衡。匹配队列包括2576例MoMHR翻修手术,每个研究组包括1288例翻修手术(两组平均随访3年;范围1 - 7年)。使用单变量回归分析比较匹配组之间的术中并发症、死亡率和再次翻修手术情况。对于每个特定的非ARMD翻修指征,计算非ARMD组的植入物生存率,随后使用Cox回归分析将每个个体的非ARMD指征与ARMD组的植入物生存率进行比较。
ARMD和非ARMD的MoMHR翻修手术在术中并发症方面无差异(优势比,0.97;95%置信区间[CI],0.59 - 1.59;p = 0.900)。与非ARMD翻修相比,ARMD翻修后的死亡率较低(风险比[HR],0.43;CI,0.21 - 0.87;p = 0.019);然而,当从非ARMD指征组中排除因感染进行的翻修时,差异无统计学意义(HR,0.69;CI,0.35 - 1.37;p = 0.287)。与非ARMD翻修相比,ARMD翻修后的再次翻修率较低(HR,0.52;CI,0.36 - 0.75;p < 0.001);即使排除因感染进行的翻修后,这种差异仍然存在(HR,0.59;CI,0.40 - 0.89;p = 0.011)。与因ARMD进行的翻修(5年生存率 = 94%;CI,92% - 96%)相比,因感染进行的翻修(5年生存率 = 81%;CI,55% - 93%;p = 0.003)和脱位/半脱位进行的翻修(5年生存率 = 82%;CI,69% - 90%;p < 0.001)的植入物生存率最低。
与之前的观察结果相反,因ARMD进行MoMHR翻修的再次翻修风险约为非ARMD翻修的一半。我们怀疑全球监管机构通过建议外科医生采用较低的翻修阈值,对ARMD翻修后的再次翻修率产生了积极影响,并且此类翻修现在正在更早阶段进行。MoMHR翻修后因感染和脱位导致的再次翻修风险较高令人担忧。非ARMD翻修后观察到的死亡率增加是由感染性MoMHR翻修引起的,这与非MoMHR感染性翻修的结果相似。
III级,治疗性研究。