Medicine 1 Department, Centro Hospitalar Lisboa Norte, Lisbon, Portugal
Cardiology Department, Reference Center on Lysosomal Storage Disorders, Hospital Senhora da Oliveira, Guimarães, Portugal.
J Am Heart Assoc. 2018 Mar 13;7(6):e007124. doi: 10.1161/JAHA.117.007124.
Cardiomyopathy is a major determinant of overall Fabry disease (FD) prognosis, with the worst outcomes in patients with myocardial fibrosis. Late gadolinium enhancement is currently the gold standard for evaluation of replacement myocardial fibrosis; however, this event is irreversible, thus identification of biomarkers of earlier diffuse fibrosis is paramount.
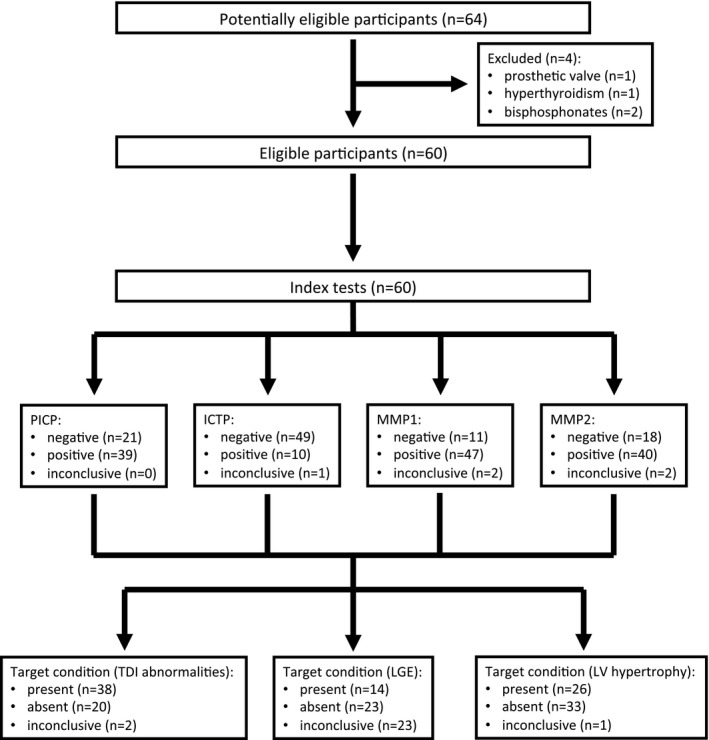
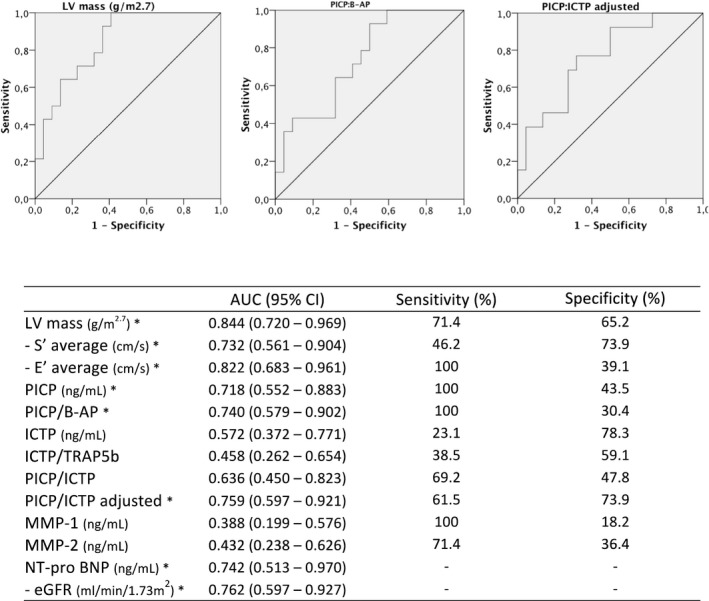
Type I collagen synthesis and degradation biomarkers (PICP [carboxyterminal propeptide of procollagen type I], ICTP [carboxyterminal telopeptide of type I collagen], and MMP1 [matrix metalloproteinase 1] and MMP2) and markers of bone synthesis and degradation were evaluated (to adjust type I collagen metabolism to bone turnover) in FD patients and controls. FD patients were grouped by cardiomyopathy severity, according to echocardiogram: (1) normal, (2) tissue Doppler abnormalities, (3) left ventricular hypertrophy. A significant increase in PICP and a significant decrease in matrix metalloproteinases were observed in FD patients; even the group with normal echocardiogram had a significant increase in PICP. We also found a significant correlation between left ventricular mass and PICP (ρ=0.378, =0.003) and MMP1 (ρ=-0.484, <0.001). PICP (adjusted for bone turnover) was the better predictor of left ventricular mass in multivariable regression, and its diagnostic accuracy to predict late gadolinium enhancement was also significant.
Collagen type I synthesis is increased in FD cardiomyopathy, even in the earlier stages of the disease, and this profibrotic state has good predictive value for and is likely to be critical to the development of overt left ventricular hypertrophy. Moreover, inhibition of enzymes involved in collagen type I cleavage also seems crucial to myocardial collagen deposition.
心肌病是法布瑞氏病(FD)整体预后的主要决定因素,心肌纤维化患者的预后最差。钆延迟增强目前是评估替代型心肌纤维化的金标准;然而,这种病变是不可逆转的,因此识别早期弥漫性纤维化的生物标志物至关重要。
在 FD 患者和对照组中评估了 I 型胶原合成和降解生物标志物(PICP[I 型前胶原羧基端肽]、ICTP[I 型胶原羧基端肽]和 MMP1[基质金属蛋白酶 1]和 MMP2)以及骨合成和降解标志物(以调整 I 型胶原代谢以适应骨转换)。根据超声心动图将 FD 患者分为以下三组:(1)正常,(2)组织多普勒异常,(3)左心室肥厚。FD 患者的 PICP 显著增加,基质金属蛋白酶显著减少;即使是超声心动图正常的组,PICP 也显著增加。我们还发现左心室质量与 PICP(ρ=0.378,=0.003)和 MMP1(ρ=-0.484,<0.001)之间存在显著相关性。PICP(调整骨转换后)是多变量回归中左心室质量更好的预测因子,其预测钆延迟增强的准确性也很显著。
FD 心肌病中 I 型胶原合成增加,即使在疾病的早期阶段也是如此,这种纤维增生状态对明显左心室肥厚的发生有很好的预测价值,并且可能对其的发展至关重要。此外,抑制参与 I 型胶原裂解的酶似乎对心肌胶原沉积也很重要。