Department of General Anesthesiology, Anesthesiology Institute, Cleveland Clinic, Cleveland, OH, United States.
Department of Outcomes Research, Anesthesiology Institute, Cleveland Clinic, Cleveland, OH, United States; Department of Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH, United States.
J Clin Anesth. 2018 Jun;47:12-18. doi: 10.1016/j.jclinane.2018.03.005. Epub 2018 Mar 12.
Epidural analgesia may be associated with fewer postoperative complications and is associated with improved survival after colon cancer resection. This study used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) to assess any association between epidural analgesia (versus non-epidural) and complications after colectomy.
Retrospective cohort study.
603 hospitals in the United States reporting data to NSQIP.
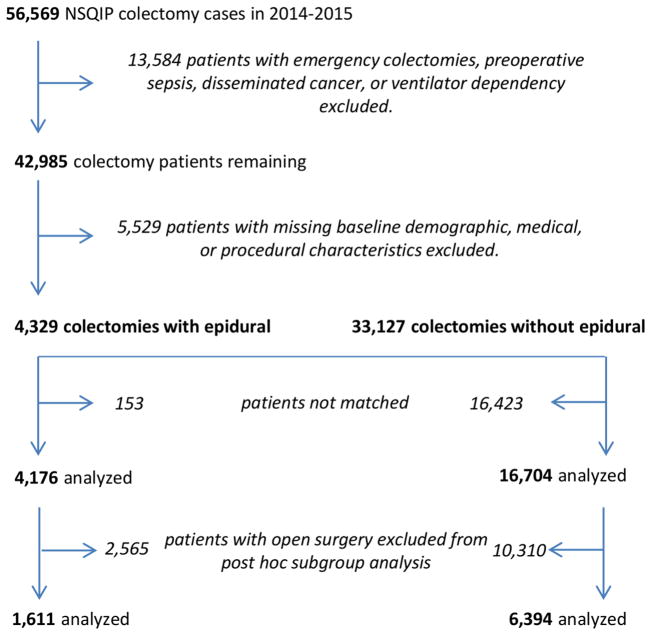
From 2014-15 data, 4176 patients undergoing colectomy with records indicating epidural analgesia were matched 1:4 via propensity scores to 16,704 patients without.
None (observational study).
Primarily, we assessed the association between epidural analgesia and a composite of cardiopulmonary complications using an average relative effect generalized estimating equations model. Secondary outcomes included neurologic, renal, and surgical complications and length of hospitalization. Sensitivity analyses repeated the analyses on a subgroup of only open colectomies.
We found no association between epidural analgesia and the primary outcome: average relative effect (95% CI) 0.87 (0.68, 1.11); P = 0.25. We found no significant associations with any secondary outcomes. In the 8005 open colectomies, however, there was a significant association between epidural analgesia and fewer cardiopulmonary complications (average relative effect odds ratio [95% CI] of 0.58 [0.35, 0.95]; P = 0.03) and shortened hospital stay (HR for time to discharge [98.75% CI] of 1.10 [1.02, 1.18]; P < 0.001).
We found no overall association between epidural analgesia and reduced complications after colectomy. In open colectomies, however, epidural analgesia was associated with fewer cardiopulmonary complications and shorter hospitalization. This may inform analgesic choice when planning open colectomy.
硬膜外镇痛可能与较少的术后并发症相关,并与结肠癌切除术后的生存率提高相关。本研究使用美国外科医师学院国家外科质量改进计划(NSQIP)评估硬膜外镇痛(与非硬膜外镇痛相比)与结肠切除术后并发症之间的任何关联。
回顾性队列研究。
美国向 NSQIP 报告数据的 603 家医院。
从 2014-15 年的数据中,有 4176 例接受结肠切除术且记录表明使用硬膜外镇痛的患者通过倾向评分与 16704 例未使用硬膜外镇痛的患者进行 1:4 匹配。
无(观察性研究)。
主要是,我们使用平均相对效应广义估计方程模型评估硬膜外镇痛与心肺并发症综合指标之间的关联。次要结局包括神经、肾脏和手术并发症以及住院时间。敏感性分析在仅开腹结肠切除术的亚组中重复分析。
我们没有发现硬膜外镇痛与主要结局之间存在关联:平均相对效应(95%CI)为 0.87(0.68,1.11);P=0.25。我们没有发现与任何次要结局存在显著关联。然而,在 8005 例开腹结肠切除术患者中,硬膜外镇痛与较少的心肺并发症显著相关(硬膜外镇痛的平均相对效应比值比[95%CI]为 0.58[0.35,0.95];P=0.03),并且住院时间缩短(出院时间的 HR [98.75%CI]为 1.10[1.02,1.18];P<0.001)。
我们没有发现硬膜外镇痛与结肠切除术后并发症减少之间的总体关联。然而,在开腹结肠切除术患者中,硬膜外镇痛与较少的心肺并发症和较短的住院时间相关。这可能为计划开腹结肠切除术时的镇痛选择提供信息。