Papageorge Christina M, Zhao Qianqian, Foley Eugene F, Harms Bruce A, Heise Charles P, Carchman Evie H, Kennedy Gregory D
Department of Surgery, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin.
Department of Biostatistics and Medical Informatics, University of Wisconsin-Madison, Madison, Wisconsin.
J Surg Res. 2016 Jul;204(1):83-93. doi: 10.1016/j.jss.2016.04.020. Epub 2016 Apr 22.
Laparoscopic and open approaches to colon resection have equivalent long-term outcomes and oncologic integrity for the treatment of colon cancer. Differences in short-term outcomes should therefore help to guide surgeons in their choice of operation. We hypothesized that minimally invasive colectomy is associated with superior short-term outcomes compared to traditional open colectomy in the setting of colon cancer.
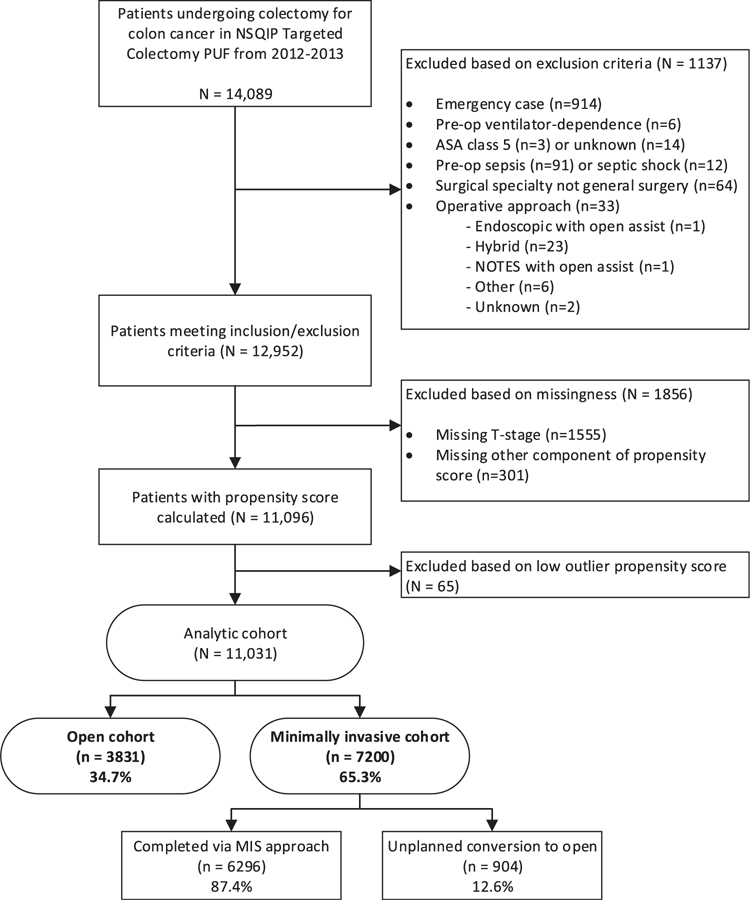
Patients undergoing nonemergent colectomy for colon cancer in 2012 and 2013 were selected from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) targeted colectomy participant use file. Patients were divided into two cohorts based on operative approach-open versus minimally invasive surgery (MIS). Univariate, multivariate, and propensity-adjusted multivariate analyses were performed to compare postoperative outcomes between the two groups.
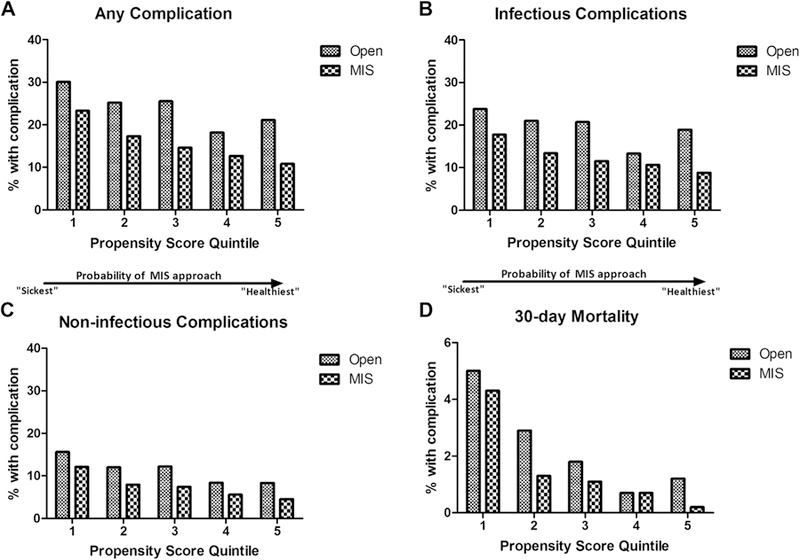
A total of 11,031 patients were identified for inclusion in the study, with an overall MIS rate of 65.3% (n = 7200). On both univariate and multivariate analysis, MIS approach was associated with fewer postoperative complications and lower mortality. In the risk-adjusted multivariate analysis, MIS approach was associated with an odds ratio of 0.598 for any postoperative morbidity compared to open (P < 0.001).
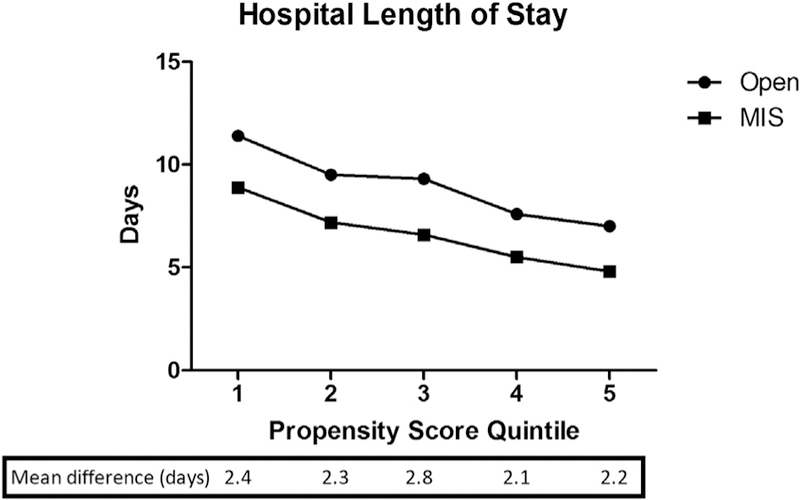
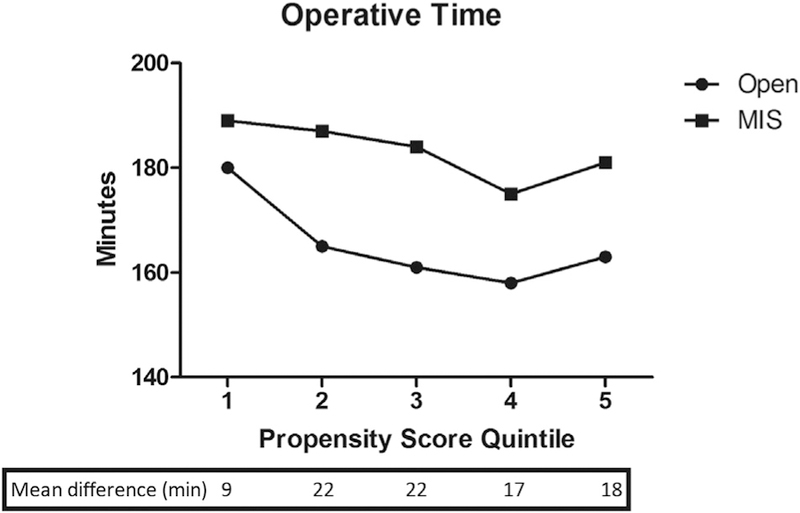
This retrospective study of patients undergoing colectomy for colon cancer demonstrates significantly improved outcomes associated with a MIS approach, even when controlling for baseline differences in illness severity. When feasible, minimally invasive colectomy should be considered gold standard for the surgical treatment of colon cancer.
腹腔镜和开放手术方式在结肠癌治疗中的长期疗效和肿瘤学完整性相当。因此,短期疗效的差异应有助于指导外科医生选择手术方式。我们假设,在结肠癌治疗中,与传统开放结肠切除术相比,微创结肠切除术的短期疗效更佳。
从美国外科医师学会国家外科质量改进计划(ACS-NSQIP)目标结肠切除术参与者使用文件中选取2012年和2013年因结肠癌接受非急诊结肠切除术的患者。根据手术方式将患者分为两组——开放手术组与微创外科手术(MIS)组。进行单因素、多因素和倾向调整多因素分析以比较两组术后结果。
共确定11031例患者纳入研究,总体MIS率为65.3%(n = 7200)。单因素和多因素分析均显示,MIS手术方式术后并发症更少,死亡率更低。在风险调整多因素分析中,与开放手术相比,MIS手术方式任何术后发病的比值比为0.598(P < 0.001)。
这项对因结肠癌接受结肠切除术患者的回顾性研究表明,即使在控制疾病严重程度的基线差异后,MIS手术方式的疗效仍显著改善。在可行的情况下,微创结肠切除术应被视为结肠癌手术治疗的金标准。