Wang Xiaoqing, Bai Yang, Cui Mangmang, Zhang Qingxiang, Zhang Wei, Fang Feng, Song Tianqiang
Department of Hepatobiliary Oncology, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer; Key Laboratory of Cancer Prevention and Therapy, Tianjin; Tianjin's Clinical Research Center for Cancer, Tianjin 300060, China.
Cancer Biol Med. 2018 Feb;15(1):79-87. doi: 10.20892/j.issn.2095-3941.2017.0153.
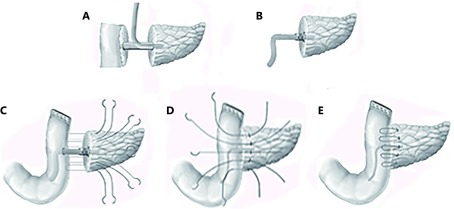
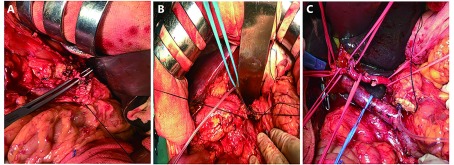
This study proposed a modified Blumgart anastomosis (m-BA) that uses a firm ligation of the main pancreatic duct with a supporting tube to replace the pancreatic duct-to-jejunum mucosa anastomosis, with the aim of simplifying the complicated steps of the conventional BA (c-BA). Thus, we observe if a difference in the risk of postoperative pancreatic fistula (POPF) exists between the two methods.
The m-BA anastomosis method has been used since 2010. From October 2011 to October 2015, 147 patients who underwent pancreatoduodenectomy (PD) using BA in Tianjin Medical University Cancer Institute and Hospital were enrolled in this study. According to the type of pancreatojejunostomy (PJ), 50 patients underwent m-BA and 97 received c-BA. The two patient cohorts were compared prospectively to some extent but not randomized, and the evaluated variables were operation time, the incidence rate of POPF, and other perioperative complications.
The operation time showed no significant difference ( > 0.05) between the two groups, but the time of duct-to-mucosa anastomosis in the m-BA group was much shorter than that in the c-BA group ( < 0.001). The incidence rate of clinically relevant POPF was 12.0% (6/50) in the modified group and 10.3% (10/97) in the conventional group ( > 0.05), which means that the modified anastomosis method did not cause additional pancreatic leakage. The mean length of postoperative hospital stay of the m-BA group was 23 days, and that of the c-BA group was 22 days ( > 0.05).
Compared with the conventional BA, we suggest that the modified BA is a feasible, safe, and effective operation method for P J of PD with no sacrifice of surgical quality. In the multivariate analysis, we also found that body mass index (≥ 25 kg/m) increased the risk of POPF.
本研究提出一种改良的布卢姆加特吻合术(m - BA),该方法通过牢固结扎主胰管并使用支撑管来替代胰管与空肠黏膜吻合,旨在简化传统布卢姆加特吻合术(c - BA)的复杂步骤。因此,我们观察这两种方法在术后胰瘘(POPF)风险上是否存在差异。
自2010年起采用m - BA吻合方法。2011年10月至2015年10月,天津医科大学肿瘤医院147例行胰十二指肠切除术(PD)并采用布卢姆加特吻合术的患者纳入本研究。根据胰空肠吻合术(PJ)类型,50例患者接受m - BA,97例接受c - BA。两组患者在一定程度上进行了前瞻性比较但未随机分组,评估变量包括手术时间、POPF发生率及其他围手术期并发症。
两组手术时间无显著差异(P>0.05),但m - BA组胰管与黏膜吻合时间明显短于c - BA组(P<0.001)。改良组临床相关POPF发生率为12.0%(6/50),传统组为10.3%(10/97)(P>0.05),这意味着改良吻合方法未导致额外的胰漏。m - BA组术后平均住院时间为23天,c - BA组为22天(P>0.05)。
与传统的布卢姆加特吻合术相比,我们认为改良的布卢姆加特吻合术是一种可行、安全且有效的胰十二指肠切除术胰空肠吻合术操作方法,且不牺牲手术质量。在多因素分析中,我们还发现体重指数(≥25kg/m²)会增加POPF的风险。