Laboratory of Neurochemistry, Neurology Department, Centro Hospitalar e Universitário de Coimbra, 3000-075, Coimbra, Portugal.
Center for Neuroscience and Cell Biology, University of Coimbra, 3004-504, Coimbra, Portugal.
Alzheimers Res Ther. 2018 Mar 20;10(1):33. doi: 10.1186/s13195-018-0362-2.
Cerebrospinal fluid (CSF) biomarkers have been used to increase the evidence of underlying Alzheimer's disease (AD) pathology in mild cognitive impairment (MCI). However, CSF biomarker-based classification often results in conflicting profiles with controversial prognostic value. Normalization of the CSF Aβ42 concentration to the level of total amyloid beta (Aβ), using the Aβ42/40 ratio, has been shown to improve the distinction between AD and non-AD dementia. Therefore, we evaluated whether the Aβ42/40 ratio would improve MCI categorization and more accurately predict progression to AD.
Our baseline population consisted of 197 MCI patients, of which 144 had a follow-up ≥ 2 years, and comprised the longitudinal study group. To establish our own CSF Aβ42/40 ratio reference value, a group of 168 AD-dementia patients and 66 neurological controls was also included. CSF biomarker-based classification was operationalized according to the framework of the National Institute of Aging-Alzheimer Association criteria for MCI.
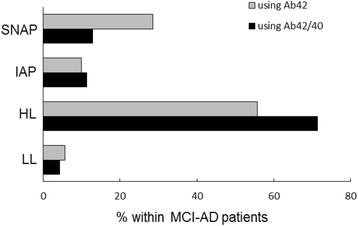
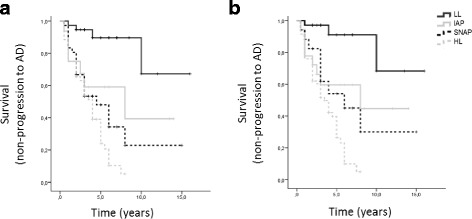
When using the core CSF biomarkers (Aβ42, total Tau and phosphorylated Tau), 30% of the patients fell into the high-AD-likelihood (HL) group (both amyloid and neurodegeneration markers positive), 30% into the low-AD-likelihood group (all biomarkers negative), 28% into the suspected non-Alzheimer pathophysiology (SNAP) group (only neurodegeneration markers positive) and 12% into the isolated amyloid pathology group (only amyloid-positive). Replacing Aβ42 by the Aβ42/40 ratio resulted in a significant increase in the percentage of patients with amyloidosis (42-59%) and in the proportion of interpretable biological profiles (61-75%), due to a reduction by half in the number of SNAP cases and an increase in the proportion of the HL subgroup. Survival analysis showed that risk of progression to AD was highest in the HL group, and increased when the Aβ42/40 ratio, instead of Aβ42, combined with total Tau and phosphorylated Tau was used for biomarker-based categorization.
Our results confirm the usefulness of the CSF Aβ42/40 ratio in the interpretation of CSF biomarker profiles in MCI patients, by increasing the proportion of conclusive profiles and enhancing their predictive value for underlying AD.
脑脊液(CSF)生物标志物已被用于增加轻度认知障碍(MCI)患者潜在阿尔茨海默病(AD)病理的证据。然而,基于 CSF 生物标志物的分类通常会导致具有争议预后价值的冲突模式。通过使用 Aβ42/40 比值将 CSF Aβ42 浓度归一化为总淀粉样β(Aβ)水平,已显示出可以改善 AD 与非 AD 痴呆之间的区分。因此,我们评估了 Aβ42/40 比值是否会改善 MCI 的分类,并更准确地预测向 AD 的进展。
我们的基线人群由 197 名 MCI 患者组成,其中 144 名患者的随访时间≥2 年,组成了纵向研究组。为了建立我们自己的 CSF Aβ42/40 比值参考值,还纳入了 168 名 AD 痴呆患者和 66 名神经科对照组。根据美国国家老龄化研究所-阿尔茨海默病协会(NIA-AA)MCI 标准的框架,实施基于 CSF 生物标志物的分类。
当使用核心 CSF 生物标志物(Aβ42、总 Tau 和磷酸化 Tau)时,30%的患者归入高 AD 可能性(HL)组(淀粉样和神经退行性标记物均阳性),30%归入低 AD 可能性组(所有生物标志物均阴性),28%归入疑似非阿尔茨海默病病理生理学(SNAP)组(仅神经退行性标记物阳性),12%归入孤立淀粉样病理学组(仅淀粉样阳性)。用 Aβ42/40 比值代替 Aβ42,由于 SNAP 病例数减少一半,以及 HL 亚组的比例增加,导致淀粉样病患者的比例(42-59%)和可解释的生物学谱比例(61-75%)显著增加。生存分析表明,HL 组向 AD 进展的风险最高,当使用 Aβ42/40 比值结合总 Tau 和磷酸化 Tau 进行基于生物标志物的分类时,这种风险会增加。
我们的结果证实了 CSF Aβ42/40 比值在解释 MCI 患者 CSF 生物标志物谱中的有用性,通过增加明确谱的比例并增强其对潜在 AD 的预测价值。