Sacoor Mohamed F
Department of Dermatology, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
South Afr J HIV Med. 2017 Apr 28;18(1):693. doi: 10.4102/sajhivmed.v18i1.693. eCollection 2017.
Histoplasmosis is a systemic mycosis caused by the dimorphic fungus . We report a case of disseminated cutaneous histoplasmosis with mucocutaneous involvement in an AIDS patient paradigmatic of the multifaceted nature of the disease, which is an expression of the immune reconstitution inflammatory syndrome (IRIS).
A 39-year-old man presented with a three month history of asymptomatic papules and nodules with necrotic centres involving the centrofacial region. The patient was diagnosed as being HIV-positive a month earlier and was commenced on antiretroviral treatment. Two weeks after the development of skin lesions, the patient complained of a sore throat and hoarseness of his voice. A fibre-optic laryngoscopy and biopsies of the skin, larynx and liver were performed.
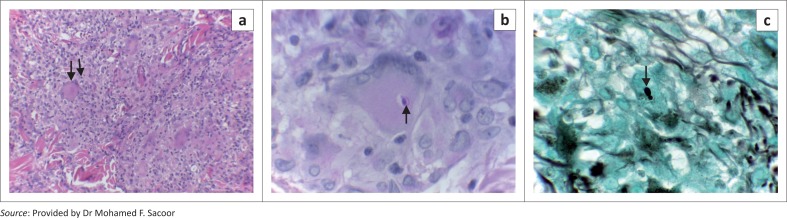
The CD4 counts increased from 2 cells/µL to 124 cells/µL, whereas the viral load decreased from one million to less than 20 copies/mL. A fibre-optic laryngoscopy revealed a supraglottitis with ulceration on the epiglottis. Histology of the liver, larynx and sections of the skin demonstrated pandermal necrotising granulomatous inflammation. Grocott-Gomori methenamine silver and Periodic acid-Schiff (PAS) stains revealed a relative paucity of intracellular, narrow-neck budding fungal organisms. Culture findings confirmed the diagnosis of histoplasmosis. The patient was treated with intravenous amphotericin B for two weeks followed by oral itraconazole 100 mg twice a day, with an excellent response to treatment.
We present this case to remind clinicians that disseminated histoplasmosis in AIDS patients may occur as an expression of IRIS. A sudden onset of hoarseness with cutaneous lesions in a patient with disseminated disease should alert one to possible laryngeal histoplasmosis. Prompt recognition and treatment will avert the potential fatal complications of this disease.
组织胞浆菌病是一种由双相真菌引起的全身性真菌病。我们报告一例艾滋病患者发生播散性皮肤组织胞浆菌病并伴有黏膜皮肤受累的病例,该病例体现了该病多方面的性质,是免疫重建炎症综合征(IRIS)的一种表现。
一名39岁男性,有三个月无症状丘疹和结节病史,中央面部区域出现坏死中心。该患者一个月前被诊断为HIV阳性,并开始接受抗逆转录病毒治疗。皮肤病变出现两周后,患者主诉喉咙痛和声音嘶哑。进行了纤维喉镜检查以及皮肤、喉部和肝脏活检。
CD4细胞计数从2个/微升增加到124个/微升,而病毒载量从100万降至低于20拷贝/毫升。纤维喉镜检查显示会厌上炎伴会厌溃疡。肝脏、喉部和皮肤切片的组织学检查显示全层坏死性肉芽肿性炎症。格罗特-高莫里六胺银染色和过碘酸希夫(PAS)染色显示细胞内窄颈芽生真菌生物体相对较少。培养结果确诊为组织胞浆菌病。患者接受了两周的静脉注射两性霉素B治疗,随后口服伊曲康唑,每天两次,每次100毫克,治疗反应良好。
我们报告此病例以提醒临床医生,艾滋病患者的播散性组织胞浆菌病可能作为IRIS的一种表现出现。患有播散性疾病的患者突然出现声音嘶哑和皮肤病变应提醒警惕可能的喉部组织胞浆菌病。及时识别和治疗将避免该病潜在的致命并发症。