Johnson Leigh F, Dorrington Rob E, Moolla Haroon
Centre for Infectious Disease Epidemiology and Research, University of Cape Town, South Africa.
Centre for Actuarial Research, University of Cape Town, South Africa.
South Afr J HIV Med. 2017 Jul 28;18(1):695. doi: 10.4102/sajhivmed.v18i1.695. eCollection 2017.
HIV prevalence differs substantially between South Africa's provinces, but the factors accounting for this difference are poorly understood.
To estimate HIV prevalence and incidence trends by province, and to identify the epidemiological factors that account for most of the variation between provinces.
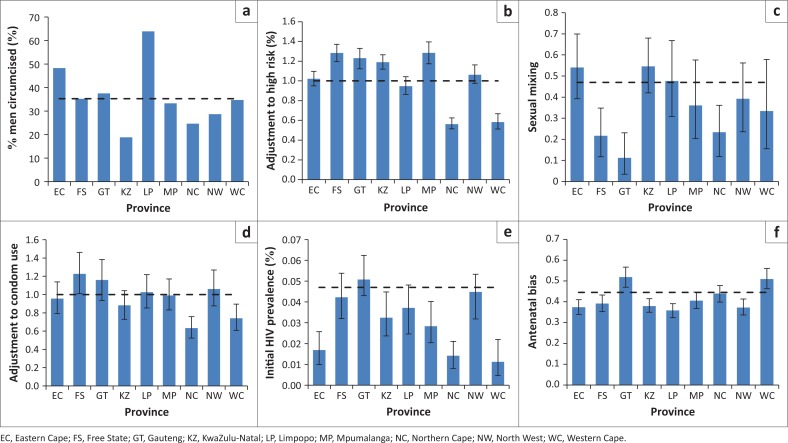
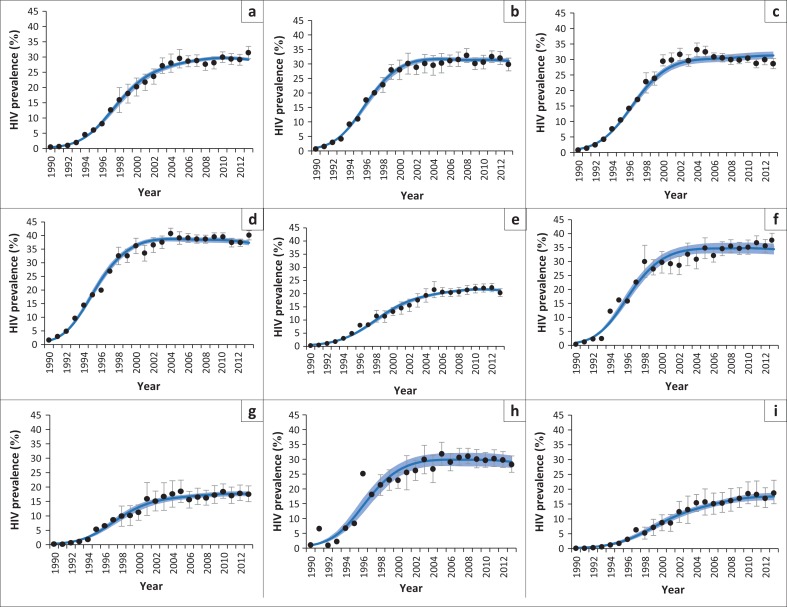
A mathematical model of the South African HIV epidemic was applied to each of the nine provinces, allowing for provincial differences in demography, sexual behaviour, male circumcision, interventions and epidemic timing. The model was calibrated to HIV prevalence data from antenatal and household surveys using a Bayesian approach. Parameters estimated for each province were substituted into the national model to assess sensitivity to provincial variations.
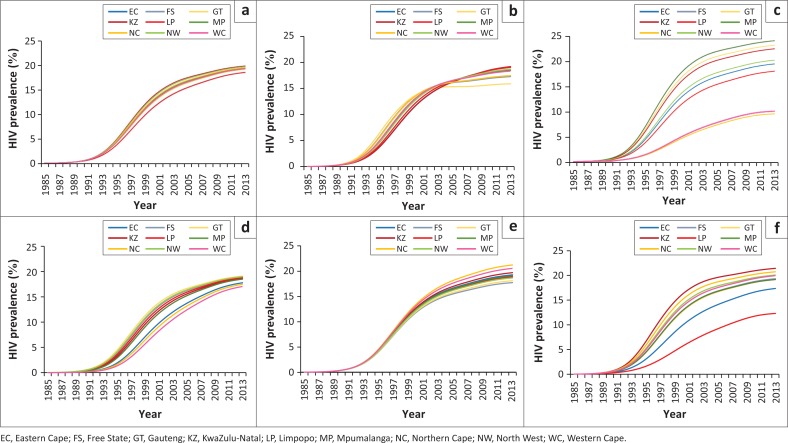
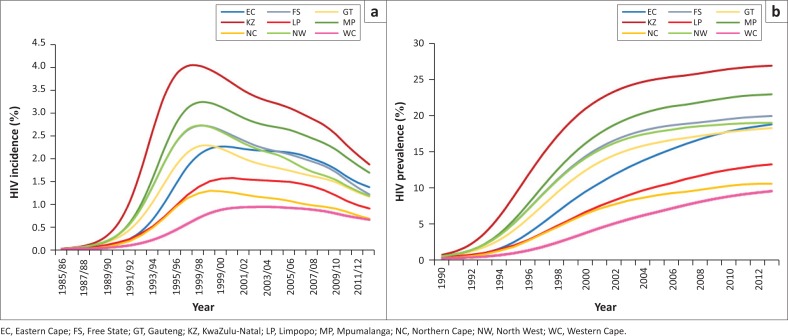
HIV incidence in 15-49-year-olds peaked between 1997 and 2003 and has since declined steadily. By mid-2013, HIV prevalence in 15-49-year-olds varied between 9.4% (95% CI: 8.5%-10.2%) in Western Cape and 26.8% (95% CI: 25.8%-27.6%) in KwaZulu-Natal. When standardising parameters across provinces, this prevalence was sensitive to provincial differences in the prevalence of male circumcision (range 12.3%-21.4%) and the level of non-marital sexual activity (range 9.5%-24.1%), but not to provincial differences in condom use (range 17.7%-21.2%), sexual mixing (range 15.9%-19.2%), marriage (range 18.2%-19.4%) or assumed HIV prevalence in 1985 (range 17.0%-19.1%).
The provinces of South Africa differ in the timing and magnitude of their HIV epidemics. Most of the heterogeneity in HIV prevalence between South Africa's provinces is attributable to differences in the prevalence of male circumcision and the frequency of non-marital sexual activity.
南非各省之间的艾滋病毒流行率差异很大,但造成这种差异的因素却鲜为人知。
估计各省的艾滋病毒流行率和发病率趋势,并确定导致各省之间大部分差异的流行病学因素。
将南非艾滋病毒流行情况的数学模型应用于九个省份中的每一个,考虑到各省在人口统计学、性行为、男性包皮环切术、干预措施和流行时间方面的差异。该模型采用贝叶斯方法根据产前和家庭调查的艾滋病毒流行率数据进行校准。将为每个省份估计的参数代入国家模型,以评估对各省差异的敏感性。
15至49岁人群的艾滋病毒发病率在1997年至2003年之间达到峰值,此后稳步下降。到2013年年中,15至49岁人群中的艾滋病毒流行率在西开普省为9.4%(95%置信区间:8.5%-10.2%),在夸祖鲁-纳塔尔省为26.8%(95%置信区间:25.8%-27.6%)。在对各省参数进行标准化时,这种流行率对各省男性包皮环切术流行率(范围为12.3%-21.4%)和非婚性行为水平(范围为9.5%-24.1%)的差异敏感,但对各省在避孕套使用(范围为17.7%-21.2%)、性混合(范围为15.9%-19.2%)、婚姻(范围为18.2%-19.4%)或1985年假定的艾滋病毒流行率(范围为17.0%-19.1%)方面的差异不敏感。
南非各省的艾滋病毒流行时间和规模存在差异。南非各省之间艾滋病毒流行率的大部分异质性可归因于男性包皮环切术流行率和非婚性行为频率的差异。