School of Medicine, College of Health Sciences, Moi University, Eldoret, Kenya.
Academic Model Providing Access to Healthcare (AMPATH), Eldoret, Kenya.
PLoS One. 2018 Mar 28;13(3):e0194047. doi: 10.1371/journal.pone.0194047. eCollection 2018.
Retention, defined as continuous engagement in care, is an important indicator for quality of healthcare services. To achieve UNAIDS 90-90-90 targets, emphasis on retention as a predictor of viral suppression in patients initiated on ART is vital. Using routinely collected clinical data, the authors sought to determine the effect of age on retention post ART initiation.
De-identified electronic data for 32965 HIV-infected persons aged ≥15 years at enrolment into the Academic Model Providing Access to Healthcare program between January 2008 and December 2014 were analyzed. Follow-up time was defined from the date of ART initiation until either loss to follow-up or death or close of the database (September 2016) was observed. Proportions were compared using Pearson's Chi-square test and medians using Mann-Whitney U test. Logistic regression model was used to assess differences in ART initiation between groups, adjusting for baseline characteristics. Cox proportional hazards model adjusting for baseline characteristics and antiretroviral therapy (ART) status was used to compute hazard ratios. Kaplan-Meier survival function was used to compare retention on ART at 12, 24, and 36 months post ART initiation.
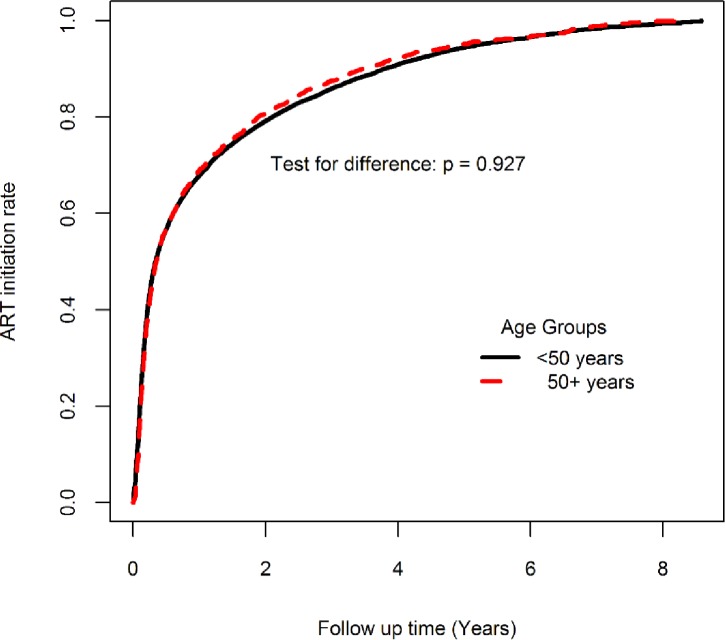
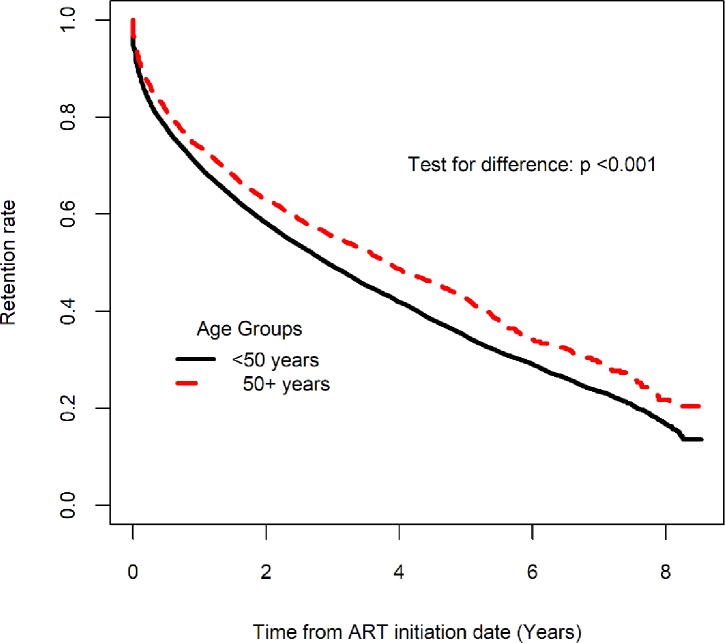
Of the total sample, 3924 (12.0%) were aged ≥50 years at enrolment. The median (IQR) age of young adults and older adults were 32.5 (26.6, 36.9) and 54.9 (51.7, 59.9) respectively. ART initiation rates were 70.5% among older adults and 68.2% among younger adults. Retention rates in care at 12, 24 and 36 months post ART initiation were 73.9% (95% CL: 72.2, 75.5), 62.9% (95% CL: 61.0, 64.7) and 55.4% (95% CL: 53.5, 57.3) among older adults compared to 69.8% (95% CL: 69.1, 70.4), 58.1% (95% CL: 57.4, 58.8) and 49.3% (95% CL: 48.6, 50.0) among younger adults (p <0.001). A higher proportion of older adults were retained in HIV care post ART initiation compared to younger adults, Adjusted Hazard Ratio (AHR): 0.83 (95% CI: 0.78, 0.87) though they were more likely to die, AHR: 1.35 (95% CI: 1.19, 1.52).
A higher proportion of older adults are initiated on ART and have better retention in care at 12, 24 and 36 months post ART initiation than younger adults. However, older adults have a higher all-cause mortality rate, perhaps partially driven by late presentation to care. Enhanced outreach and care to this group is imperative to improve their outcomes.
保留率(定义为持续参与治疗)是医疗服务质量的重要指标。为了实现联合国艾滋病规划署 90-90-90 目标,强调保留率作为接受抗逆转录病毒疗法(ART)治疗的患者病毒抑制的预测因素至关重要。作者利用常规收集的临床数据,旨在确定年龄对 ART 治疗后保留率的影响。
分析了 2008 年 1 月至 2014 年 12 月期间,学术模型提供医疗保健服务项目中年龄≥15 岁的 32965 名 HIV 感染者的匿名电子数据。随访时间从开始接受 ART 治疗之日起计算,直到随访丢失、死亡或数据库关闭(2016 年 9 月)。使用 Pearson's Chi-square 检验比较比例,使用 Mann-Whitney U 检验比较中位数。使用逻辑回归模型调整基线特征评估组间 ART 治疗的差异。使用 Cox 比例风险模型调整基线特征和抗逆转录病毒治疗(ART)状况,计算风险比。使用 Kaplan-Meier 生存函数比较 ART 治疗后 12、24 和 36 个月的保留率。
在总样本中,3924 人(12.0%)在入组时年龄≥50 岁。年轻成人和老年成人的中位数(IQR)年龄分别为 32.5(26.6,36.9)和 54.9(51.7,59.9)。老年成人和年轻成人的 ART 治疗启动率分别为 70.5%和 68.2%。ART 治疗后 12、24 和 36 个月的保留率分别为 73.9%(95% CL:72.2,75.5)、62.9%(95% CL:61.0,64.7)和 55.4%(95% CL:53.5,57.3),老年成人组与年轻成人组(p <0.001)相比,69.8%(95% CL:69.1,70.4)、58.1%(95% CL:57.4,58.8)和 49.3%(95% CL:48.6,50.0)。尽管老年成人更有可能死亡,风险比(AHR):1.35(95% CI:1.19,1.52),但与年轻成人相比,老年成人在 ART 治疗后更有可能留在 HIV 护理中,调整后的风险比(AHR):0.83(95% CI:0.78,0.87)。
与年轻成人相比,更多的老年成人开始接受 ART 治疗,并且在 ART 治疗后 12、24 和 36 个月时在护理中保留率更高。然而,老年成人的全因死亡率更高,这可能部分归因于晚期接受护理。为了改善他们的结局,需要加强对这一群体的宣传和护理。