Fatti Geoffrey, Mothibi Eula, Meintjes Graeme, Grimwood Ashraf
Kheth'Impilo, Cape Town, South Africa.
Division of Infectious Diseases and HIV Medicine, Department of Medicine, University of Cape Town, Cape Town, South Africa; Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa; Department of Medicine, Imperial College, London, United Kingdom.
PLoS One. 2014 Jun 20;9(6):e100273. doi: 10.1371/journal.pone.0100273. eCollection 2014.
Increasing numbers of patients are starting antiretroviral treatment (ART) at advanced age or reaching advanced age while on ART. We compared baseline characteristics and ART outcomes of older adults (aged ≥55 years) vs. younger adults (aged 25-54 years) in routine care settings in South Africa.
A multicentre cohort study of ART-naïve adults starting ART at 89 public sector facilities was conducted. Mortality, loss to follow-up (LTFU), immunological and virological outcomes until five years of ART were compared using competing-risks regression, generalised estimating equations and mixed-effects models.
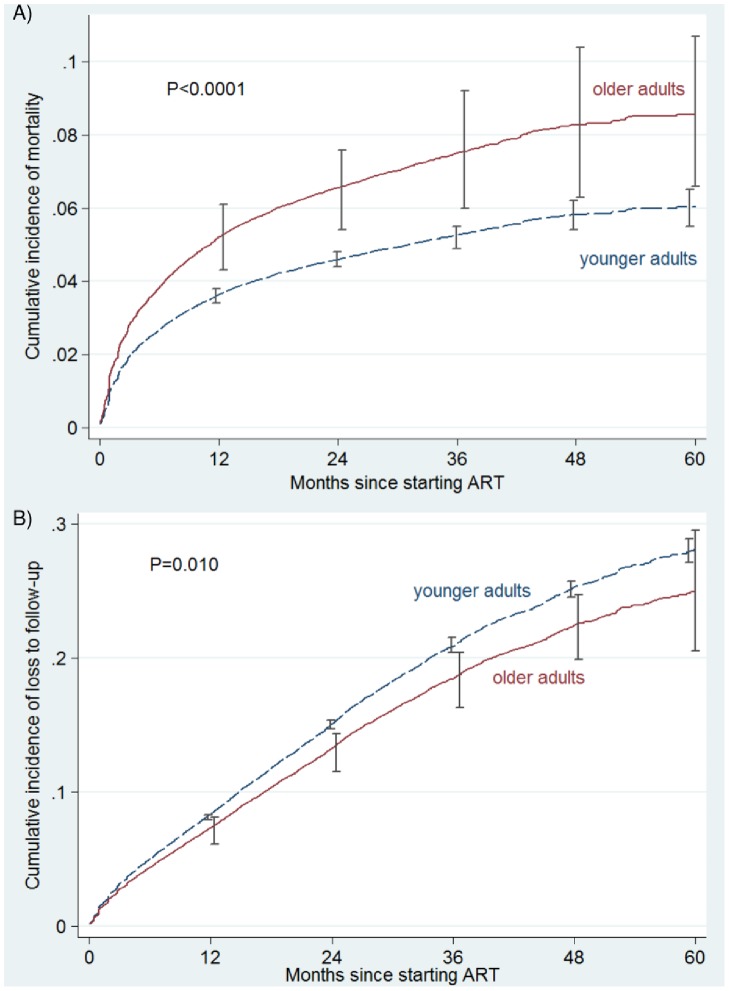
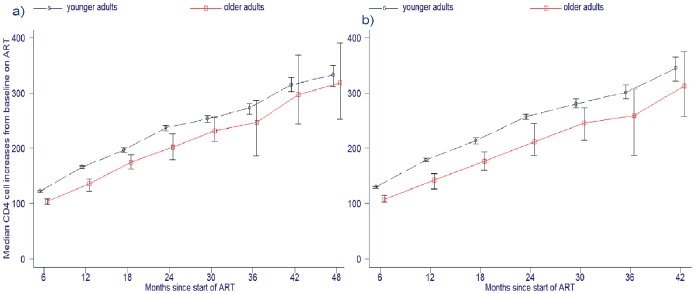
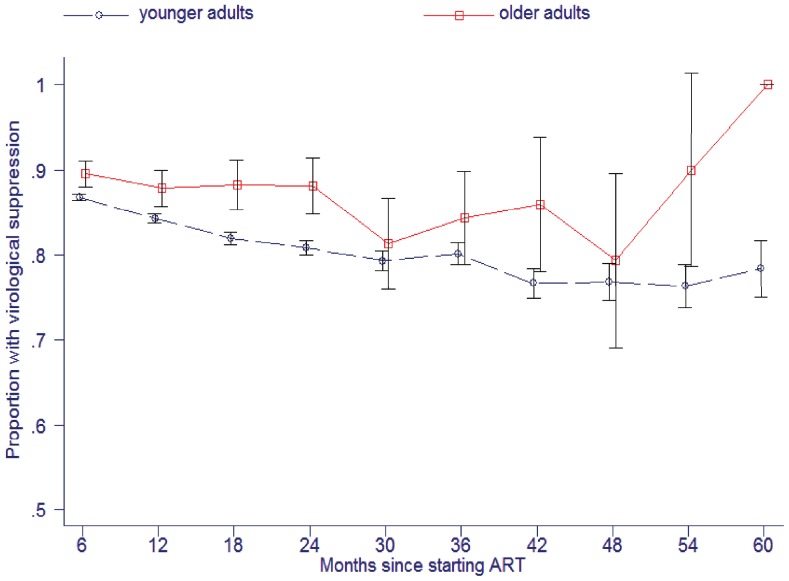
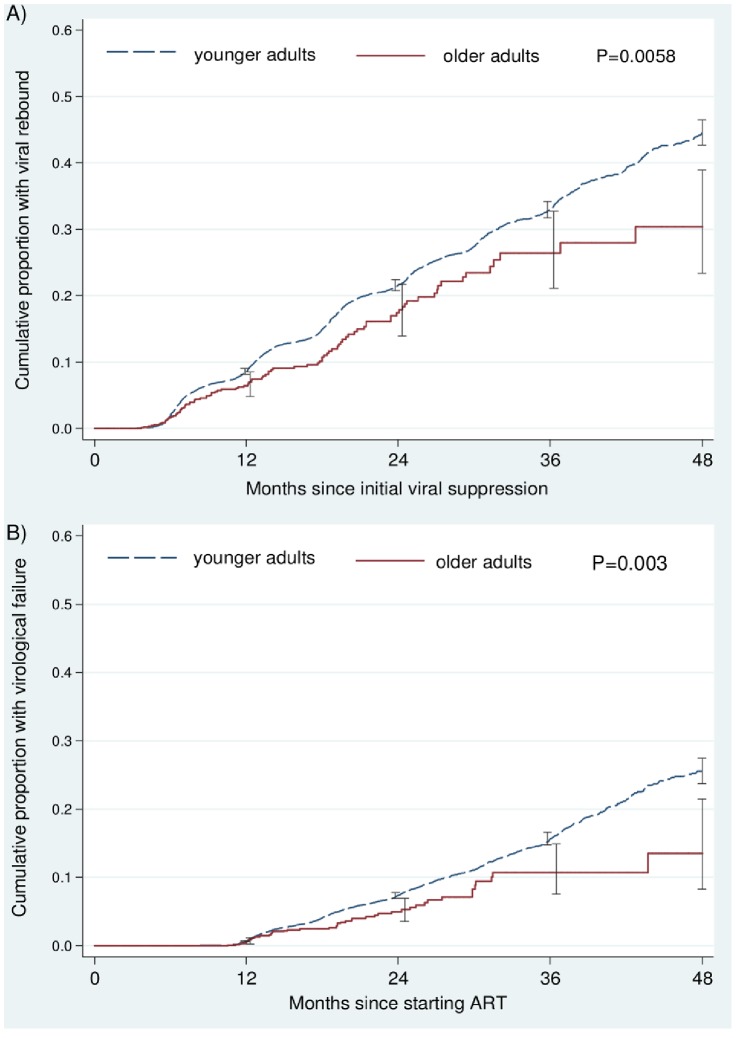
4065 older adults and 86,006 younger adults were included. There were more men amongst older adults; 44.7% vs. 33.4%; RR = 1.34 (95% CI: 1.29-1.39). Mortality after starting ART was substantially higher amongst older adults, adjusted sub-hazard ratio (asHR) = 1.44 over 5 years (95% CI: 1.26-1.64), particularly for the period 7-60 months of treatment, asHR = 1.73 (95% CI: 1.44-2.10). LTFU was lower in older adults, asHR = 0.87 (95% CI: 0.78-0.97). Achievement of virological suppression was greater in older adults, adjusted odds ratio = 1.42 (95% CI: 1.23-1.64). The probabilities of viral rebound and confirmed virological failure were both lower in older adults, adjusted hazard ratios = 0.69 (95% CI: 0.56-0.85) and 0.64 (95% CI: 0.47-0.89), respectively. The rate of CD4 cell recovery (amongst patients with continuous viral suppression) was 25 cells/6 months of ART (95% CI: 17.3-33.2) lower in older adults.
Although older adults had better virological outcomes and reduced LTFU, their higher mortality and slower immunological recovery warrant consideration of age-specific ART initiation criteria and management strategies.
越来越多的患者在高龄时开始接受抗逆转录病毒治疗(ART),或在接受ART治疗期间步入高龄阶段。我们比较了南非常规医疗环境中老年人(年龄≥55岁)与年轻人(年龄25 - 54岁)的基线特征及ART治疗结果。
对89个公共部门机构中开始接受ART治疗的初治成年患者进行了一项多中心队列研究。使用竞争风险回归、广义估计方程和混合效应模型比较了直至ART治疗五年时的死亡率、失访率(LTFU)、免疫学和病毒学结果。
纳入了4065名老年人和86006名年轻人。老年人中男性更多;分别为44.7%和33.4%;风险比(RR)=1.34(95%置信区间:1.29 - 1.39)。开始ART治疗后的死亡率在老年人中显著更高,调整后的亚风险比(asHR)在5年期间为1.44(95%置信区间:1.26 - 1.64),特别是在治疗7 - 60个月期间,asHR = 1.73(95%置信区间:1.44 - 2.10)。老年人的失访率较低,asHR = 0.87(95%置信区间:0.78 - 0.97)。老年人实现病毒学抑制的情况更好,调整后的优势比=1.42(95%置信区间:1.23 - 1.64)。老年人病毒反弹和确诊病毒学失败的概率均较低,调整后的风险比分别为0.69(95%置信区间:0.56 - 0.85)和0.64(95%置信区间:0.47 - 0.89)。老年人(在持续病毒抑制的患者中)CD4细胞恢复率比年轻人低25个细胞/6个月的ART治疗时间(95%置信区间:17.3 - 33.2)。
尽管老年人有更好的病毒学结果且失访率降低,但其较高的死亡率和较慢的免疫学恢复值得考虑针对年龄的ART启动标准和管理策略。