Department of Medicine, Stanford University, Stanford, California, United States of America.
Uganda Heart Institute, Mulago Hospital, Kampala, Uganda.
PLoS One. 2018 Mar 28;13(3):e0194030. doi: 10.1371/journal.pone.0194030. eCollection 2018.
Rheumatic heart disease (RHD) is a leading cause of premature mortality in low- and middle-income countries (LMICs). Women of reproductive age are a unique and vulnerable group of RHD patients, due to increased risk of cardiovascular complications and death during pregnancy. Yet, less than 5% of women of childbearing age with RHD in LMICs use contraceptives, and one in five pregnant women with RHD take warfarin despite known teratogenicity. It is unclear whether this suboptimal contraception and anticoagulant use during pregnancy is due to lack of health system resources, limited health literacy, or social pressure to bear children.
We conducted a mixed methods study of 75 women living with RHD in Uganda. Questionnaires were administered to 50 patients. Transcripts from three focus groups with 25 participants were analyzed using qualitative description methodology.
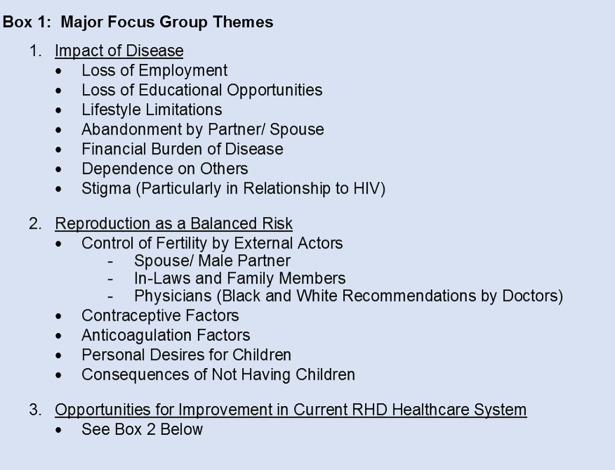
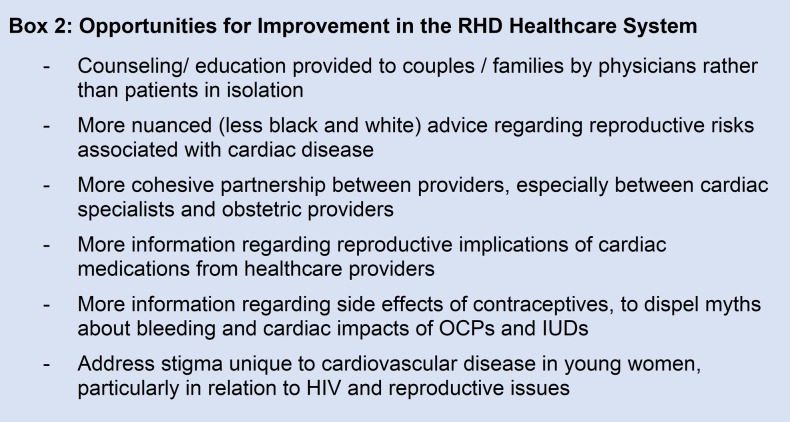
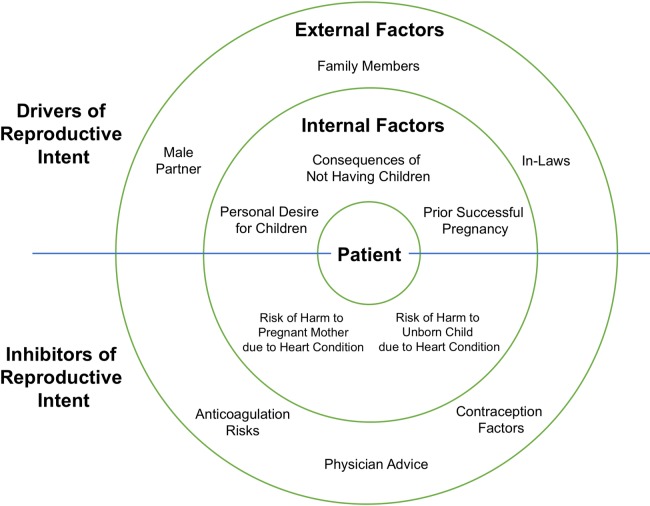
Several themes emerged from the focus groups, including pregnancy as a calculated risk; misconceptions about side-effects of contraceptives and anticoagulation; reproductive decision-making control by male partners, in-laws, or physicians; abandonment of patients by male partners; and considerable stigma against heart disease patients for both their reproductive and financial limitations (often worse than that directed against HIV patients). All questionnaire respondents were told by physicians that their hearts were not strong enough to support a pregnancy. Only 14% used contraception while taking warfarin. All participants felt that society would look poorly on a woman who cannot have children due to a heart condition.
To our knowledge, this is the first qualitative study of female RHD patients and their attitudes toward cardiovascular disorders and reproduction. Our results suggest that health programs targeting heart disease in LMICs must pay special attention to the needs of women of childbearing age. There are opportunities for improved family/societal education programs and community engagement, leading to better outcomes and patient empowerment.
风湿性心脏病(RHD)是中低收入国家(LMICs)过早死亡的主要原因。育龄期妇女是 RHD 患者中一个独特而脆弱的群体,因为她们在怀孕期间发生心血管并发症和死亡的风险增加。然而,在 LMICs 中,不到 5%的育龄期 RHD 患者使用避孕药,尽管已知华法林有致畸性,但仍有五分之一的 RHD 孕妇服用。尚不清楚这种不理想的妊娠期间避孕和抗凝使用是由于缺乏卫生系统资源、有限的健康素养还是社会压力导致生育。
我们对乌干达的 75 名 RHD 患者进行了一项混合方法研究。对 50 名患者进行了问卷调查。对 25 名参与者的 3 个焦点小组的转录本进行了定性描述方法分析。
焦点小组提出了几个主题,包括怀孕是一种有计划的风险;对避孕药和抗凝剂副作用的误解;男性伴侣、姻亲和医生对生殖决策的控制;男性伴侣对患者的抛弃;以及对心脏病患者的极大耻辱,包括对其生殖和财务限制的耻辱(往往比针对 HIV 患者的耻辱更严重)。所有接受问卷调查的患者都被医生告知,她们的心脏不够强壮,无法承受怀孕。只有 14%的人在服用华法林时使用避孕药。所有参与者都认为,由于心脏病,一个不能生育的女性会受到社会的不良评价。
据我们所知,这是第一项针对女性 RHD 患者及其对心血管疾病和生殖态度的定性研究。我们的结果表明,针对 LMICs 心脏病的卫生项目必须特别关注育龄妇女的需求。有机会改善家庭/社会教育计划和社区参与,从而改善结果和患者赋权。