Shilkofski Nicole, Crichlow Amanda, Rice Julie, Cope Leslie, Kyaw Ye Myint, Mon Thazin, Kiguli Sarah, Jung Julianna
Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Department of Emergency Medicine, University of Florida College of Medicine, Jacksonville, FL, United States.
Front Pediatr. 2018 Feb 28;6:37. doi: 10.3389/fped.2018.00037. eCollection 2018.
Under five mortality rates (UFMR) remain high for children in low- and middle-income countries (LMICs) in the developing world. Education for practitioners in these environments is a key factor to improve outcomes that will address United Nations Sustainable Development Goals 3 and 10 (good health and well being and reduced inequalities). In order to appropriately contextualize a curriculum using simulation, it is necessary to first conduct a needs assessment of the target learner population. The World Health Organization (WHO) has published a tool to assess capacity for emergency and surgical care in LMICs that is adaptable to this goal.
The WHO Tool for Situational Analysis to Assess Emergency and Essential Surgical Care was modified to assess pediatric resuscitation capacity in clinical settings in two LMICs: Uganda and Myanmar. Modifications included assessment of self-identified learning needs, current practices, and perceived epidemiology of disease burden in each clinical setting, in addition to assessment of pediatric resuscitation capacity in regard to infrastructure, procedures, equipment, and supplies. The modified tool was administered to 94 respondents from the two settings who were target learners of a proposed simulation-based curriculum in pediatric and neonatal resuscitation.
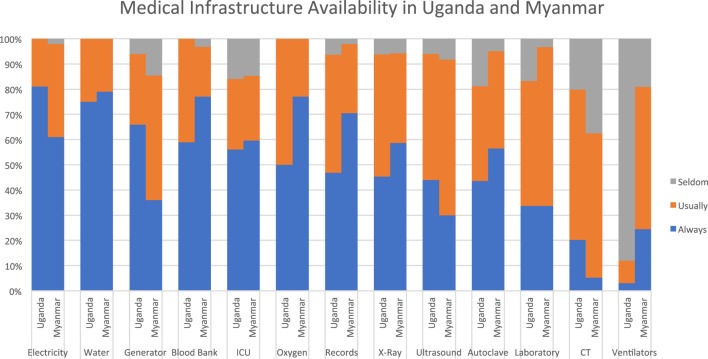
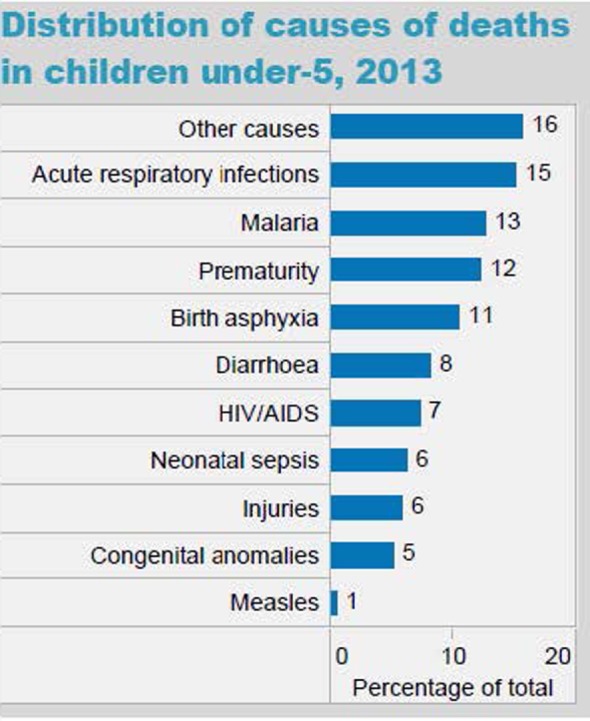
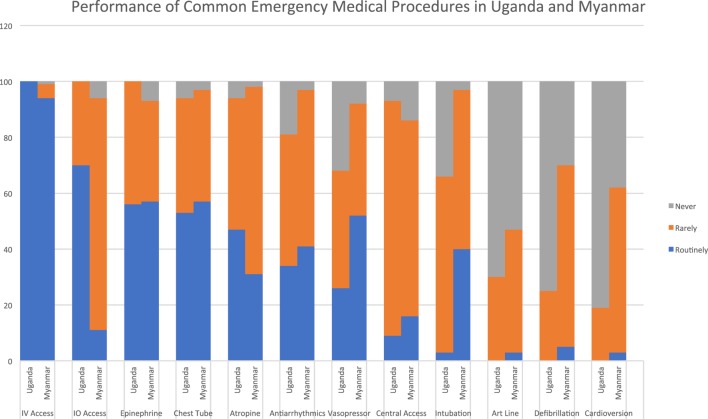
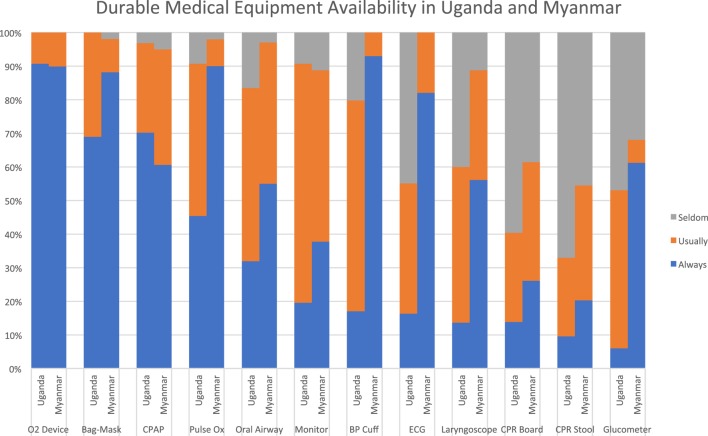
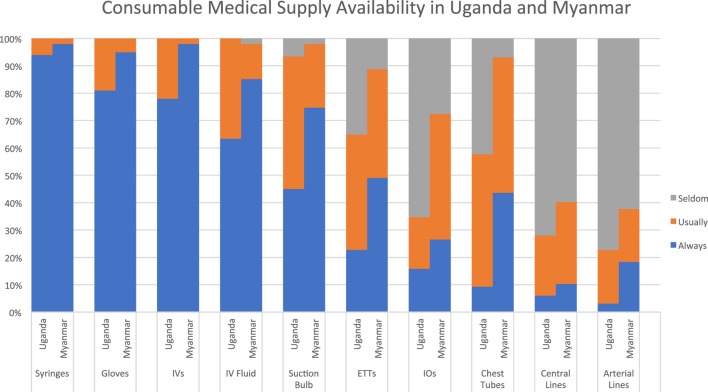
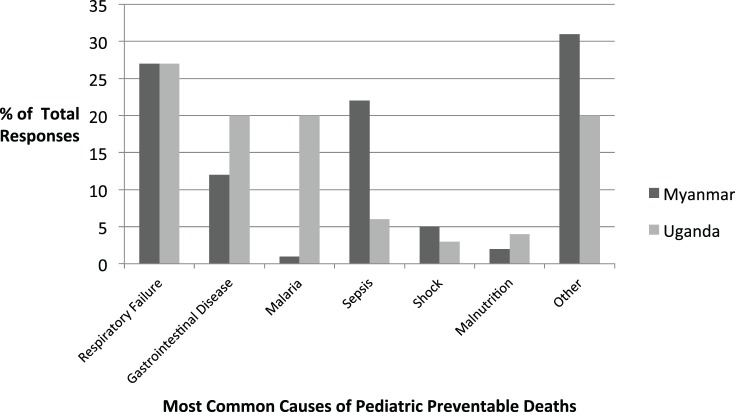
Infectious diseases (respiratory illnesses and diarrheal disease) were cited as the most common causes of pediatric deaths in both countries. Self-identified learning needs included knowledge and skill development in pediatric airway/breathing topics, as well as general resuscitation topics such as CPR and fluid resuscitation in shock. Equipment and supply availability varied substantially between settings, and critical shortages were identified in each setting. Current practices and procedures were often limited by equipment availability or infrastructural considerations.
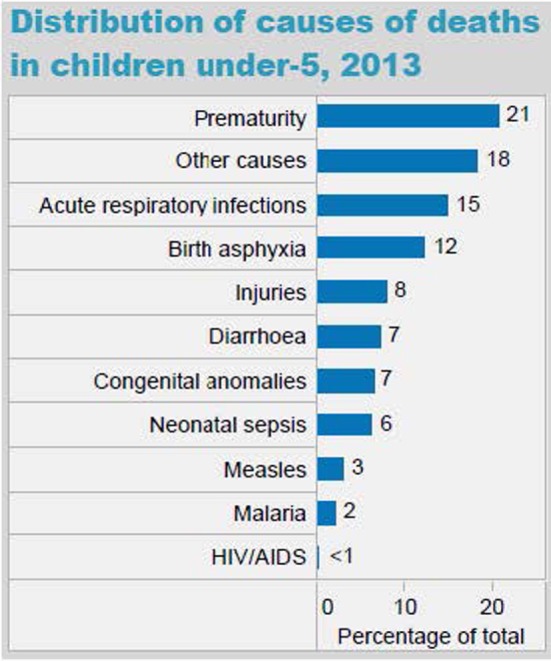
Epidemiology of disease burden reported by respondents was relatively consistent with WHO country-specific UFMR statistics in each setting. Results of the needs assessment survey were subsequently used to refine goals and objectives for the simulation curriculum and to ensure delivery of pragmatic educational content with recommendations that were contextualized for local capacity and resource availability. Effective use of the tool in two different settings increases its potential generalizability.
在发展中世界的低收入和中等收入国家(LMICs),五岁以下儿童死亡率(UFMR)仍然很高。对这些环境中的从业者进行教育是改善成果的关键因素,这将有助于实现联合国可持续发展目标3和10(良好健康与福祉以及减少不平等)。为了使用模拟对课程进行适当的情境化,首先有必要对目标学习者群体进行需求评估。世界卫生组织(WHO)发布了一种工具,可用于评估LMICs的急诊和外科护理能力,该工具适用于这一目标。
对世界卫生组织情境分析工具进行修改,以评估两个LMICs(乌干达和缅甸)临床环境中的儿科复苏能力。修改内容包括评估每个临床环境中自我确定的学习需求、当前实践以及疾病负担的感知流行病学,此外还评估儿科复苏在基础设施、程序、设备和用品方面的能力。修改后的工具应用于来自这两个环境的94名受访者,他们是拟议的儿科和新生儿复苏模拟课程的目标学习者。
传染病(呼吸道疾病和腹泻病)被认为是两国儿科死亡的最常见原因。自我确定的学习需求包括儿科气道/呼吸主题的知识和技能发展,以及诸如心肺复苏术(CPR)和休克时的液体复苏等一般复苏主题。不同环境之间的设备和用品可用性差异很大,并且在每个环境中都发现了严重短缺。当前的实践和程序通常受到设备可用性或基础设施考虑因素的限制。
受访者报告的疾病负担流行病学与每个环境中世卫组织特定国家的五岁以下儿童死亡率统计数据相对一致。需求评估调查的结果随后用于完善模拟课程的目标和目的,并确保提供符合当地能力和资源可用性的实用教育内容。该工具在两个不同环境中的有效使用增加了其潜在的通用性。