Yu Ruby, Morley John E, Kwok Timothy, Leung Jason, Cheung Osbert, Woo Jean
Department of Medicine and Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Shatin, Hong Kong.
The Chinese University of Hong Kong Jockey Club Institute of Ageing, Shatin, Hong Kong.
Front Med (Lausanne). 2018 Mar 6;5:50. doi: 10.3389/fmed.2018.00050. eCollection 2018.
To examine how various combinations of cognitive impairment (overall performance and specific domains) and pre-frailty predict risks of adverse outcomes; and to determine whether cognitive frailty may be defined as the combination of cognitive impairment and the presence of pre-frailty.
Community-based cohort study.
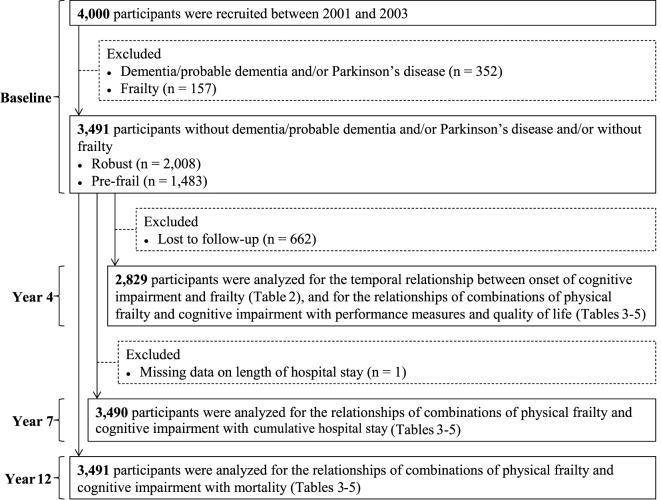
Chinese men and women ( = 3,491) aged 65+ without dementia, Parkinson's disease and/or frailty at baseline.
Frailty was characterized using the Cardiovascular Health Study criteria. Overall cognitive impairment was defined by a Cantonese Mini-Mental Status Examination (CMMSE) total score (<21/24/27, depending on participants' educational levels); delayed recall impairment by a CMMSE delayed recall score (<3); and language and praxis impairment by a CMMSE language and praxis score (<9). Adverse outcomes included poor quality of life, physical limitation, increased cumulative hospital stay, and mortality.
Compared to those who were robust and cognitively intact at baseline, those who were robust but cognitively impaired were more likely to develop pre-frailty/frailty after 4 years ( < 0.01). Compared to participants who were robust and cognitively intact at baseline, those who were pre-frail and with overall cognitive impairment had lower grip strength ( < 0.05), lower gait speed ( < 0.01), poorer lower limb strength ( < 0.01), and poorer delayed recall at year 4 [OR, 1.6; 95% confidence interval (CI), 1.2-2.3]. They were also associated with increased risks of poor quality of life (OR, 1.5; 95% CI, 1.1-2.2) and incident physical limitation at year 4 (OR, 1.8; 95% CI, 1.3-2.5), increased cumulative hospital stay at year 7 (OR, 1.5; 95% CI, 1.1-2.1), and mortality over an average of 12 years (OR, 1.5; 95% CI, 1.0-2.1) after adjustment for covariates. There was no significant difference in risks of adverse outcomes between participants who were pre-frail, with/without cognitive impairment at baseline. Similar results were obtained with delayed recall and language and praxis impairments.
Robust and cognitively impaired participants had higher risks of becoming pre-frail/frail over 4 years compared with those with normal cognition. Cognitive impairment characterized by the CMMSE overall score or its individual domain score improved the predictive power of pre-frailty for poor quality of life, incident physical limitation, increased cumulative hospital stay, and mortality. Our findings support to the concept that cognitive frailty may be defined as the occurrence of both cognitive impairment and pre-frailty, not necessarily progressing to dementia.
研究认知障碍(总体表现和特定领域)与衰弱前期的各种组合如何预测不良结局的风险;并确定认知衰弱是否可定义为认知障碍与衰弱前期并存的情况。
基于社区的队列研究。
65岁及以上的中国男性和女性(n = 3491),基线时无痴呆、帕金森病和/或衰弱。
采用心血管健康研究标准对衰弱进行特征描述。总体认知障碍由粤语简易精神状态检查表(CMMSE)总分定义(<21/24/27,取决于参与者的教育水平);延迟回忆障碍由CMMSE延迟回忆分数定义(<3);语言和实践障碍由CMMSE语言和实践分数定义(<9)。不良结局包括生活质量差、身体功能受限、累计住院时间增加和死亡率。
与基线时健康且认知完好的人相比,基线时健康但认知受损的人在4年后更有可能发展为衰弱前期/衰弱(P < 0.01)。与基线时健康且认知完好的参与者相比,衰弱前期且有总体认知障碍的参与者在第4年时握力更低(P < 0.05)、步速更低(P < 0.01)、下肢力量更差(P < 0.01),延迟回忆更差[比值比(OR),1.6;95%置信区间(CI),1.2 - 2.3]。他们还与生活质量差的风险增加(OR,1.5;95% CI,1.1 - 2.2)、第4年出现身体功能受限(OR,1.8;95% CI,1.3 - 2.5)、第7年累计住院时间增加(OR,1.5;95% CI,1.1 - 2.1)以及平均12年的死亡率增加(OR,1.5;95% CI,1.0 - 2.1)相关,在对协变量进行调整后。基线时衰弱前期且有/无认知障碍的参与者之间不良结局风险无显著差异。延迟回忆障碍以及语言和实践障碍也得到了类似结果。
与认知正常的人相比,健康但认知受损的参与者在4年内发展为衰弱前期/衰弱的风险更高。以CMMSE总分或其单个领域分数为特征的认知障碍提高了衰弱前期对生活质量差、出现身体功能受限、累计住院时间增加和死亡率的预测能力。我们的研究结果支持这样的概念,即认知衰弱可定义为认知障碍和衰弱前期的同时出现,不一定会发展为痴呆。