Division of Cardiology, Wayne State University/Detroit Medical Center, Detroit, MI
Department of Internal Medicine, Englewood Hospital and Medical Center Seton Hall University-Hackensack Meridian School of Medicine, Englewood, NJ.
J Am Heart Assoc. 2018 Apr 1;7(7):e008408. doi: 10.1161/JAHA.117.008408.
Chronic obstructive pulmonary disease (COPD) patients are at increased risk of respiratory related complications after cardiac surgery. It is unclear whether transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR) results in favorable outcomes among COPD patients.
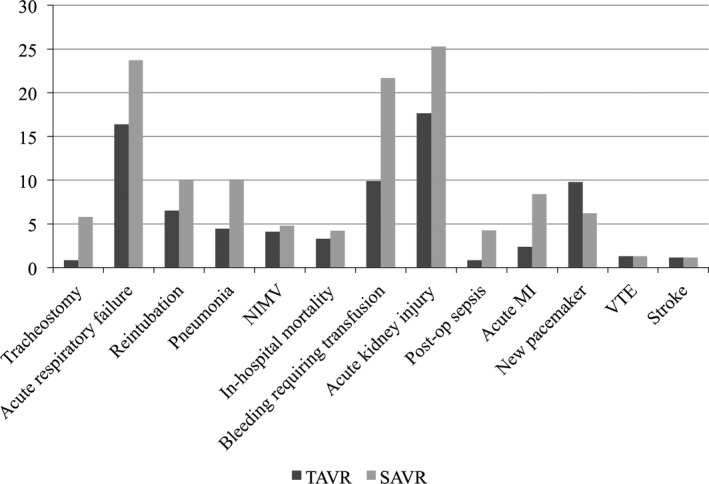
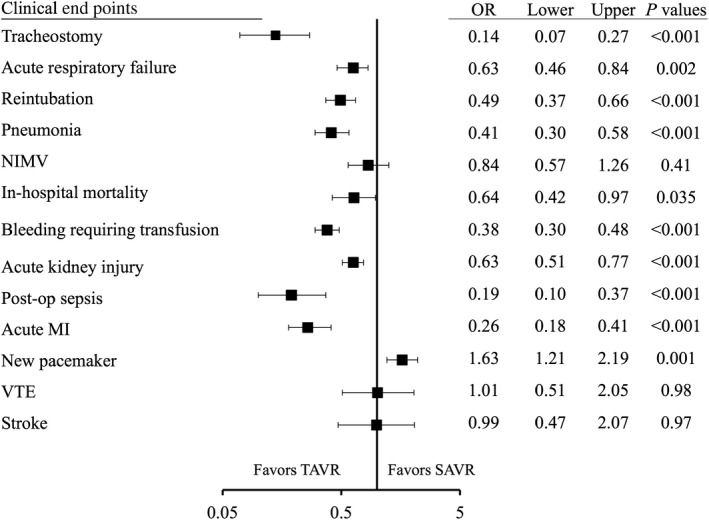
Patients were identified from the Nationwide Inpatient Sample database from 2011 to 2014. Patients with age ≥60, COPD, and either went transarterial TAVR or SAVR were included in the analysis. A 1:1 propensity-matched cohort was created to examine the outcomes. A matched pair of 1210 TAVR and 1208 SAVR patients was identified. Respiratory-related complications such as tracheostomy (0.8% versus 5.8%; odds ratio [OR], 0.14; <0.001), acute respiratory failure (16.4% versus 23.7%; OR, 0.63; =0.002), reintubation (6.5% versus 10.0%; OR, 0.49; <0.001), and pneumonia (4.5% versus 10.1%; OR, 0.41; <0.001) were significantly less frequent with TAVR versus SAVR. Use of noninvasive mechanical ventilation was similar between TAVR and SAVR (4.1% versus 4.8%; OR, 0.84; =0.41). Non-respiratory-related complications, such as in-hospital mortality (3.3% versus 4.2%; OR, 0.64; =0.035), bleeding requiring transfusion (9.9% versus 21.7%; OR, 0.38; <0.001), acute kidney injury (17.7% versus 25.3%; OR, 0.63; <0.001), and acute myocardial infarction (2.4% versus 8.4%; OR, 0.19; <0.001), were significantly less frequent with TAVR than SAVR. Cost ($56 099 versus $63 146; <0.001) and hospital stay (mean, 7.7 versus 13.0 days; <0.001) were also more favorable with TAVR than SAVR.
TAVR portended significantly fewer respiratory-related complications compared with SAVR in COPD patients. TAVR may be a preferable mode of aortic valve replacement in COPD patients.
慢性阻塞性肺疾病(COPD)患者在心脏手术后发生呼吸相关并发症的风险增加。经导管主动脉瓣置换术(TAVR)与外科主动脉瓣置换术(SAVR)相比,哪种术式更有利于 COPD 患者,目前尚不清楚。
本研究从 2011 年至 2014 年的全国住院患者样本数据库中筛选患者。纳入年龄≥60 岁、COPD 且接受经动脉 TAVR 或 SAVR 的患者进行分析。创建了 1:1 倾向评分匹配队列以检验结局。匹配了 1210 例 TAVR 患者和 1208 例 SAVR 患者。TAVR 组的气管切开术(0.8% 比 5.8%;比值比 [OR],0.14;<0.001)、急性呼吸衰竭(16.4% 比 23.7%;OR,0.63;=0.002)、再次插管(6.5% 比 10.0%;OR,0.49;<0.001)和肺炎(4.5% 比 10.1%;OR,0.41;<0.001)等呼吸系统相关并发症的发生率明显低于 SAVR 组。TAVR 与 SAVR 组的无创机械通气使用率相似(4.1% 比 4.8%;OR,0.84;=0.41)。非呼吸系统相关并发症,如院内死亡率(3.3% 比 4.2%;OR,0.64;=0.035)、需要输血的出血(9.9% 比 21.7%;OR,0.38;<0.001)、急性肾损伤(17.7% 比 25.3%;OR,0.63;<0.001)和急性心肌梗死(2.4% 比 8.4%;OR,0.19;<0.001)的发生率,TAVR 组也明显低于 SAVR 组。TAVR 的费用($56099 比 $63146;<0.001)和住院时间(均值,7.7 天比 13.0 天;<0.001)也优于 SAVR。
与 SAVR 相比,TAVR 可显著减少 COPD 患者的呼吸系统相关并发症。对于 COPD 患者,TAVR 可能是一种更优的主动脉瓣置换术式。