Willenbacher Ella, Balog Agnes, Willenbacher Wolfgang
1Internal Medicine V, Hematology & Oncology, Innsbruck Medical University, Anichstraße 35, 6020 Innsbruck, Austria.
Blood Transfusion Center, Innsbruck, Austria.
Memo. 2018;11(1):59-64. doi: 10.1007/s12254-018-0383-3. Epub 2018 Feb 21.
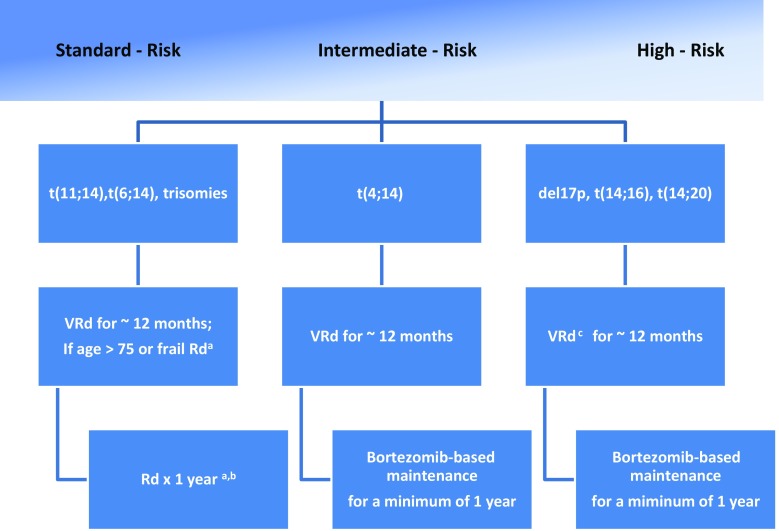
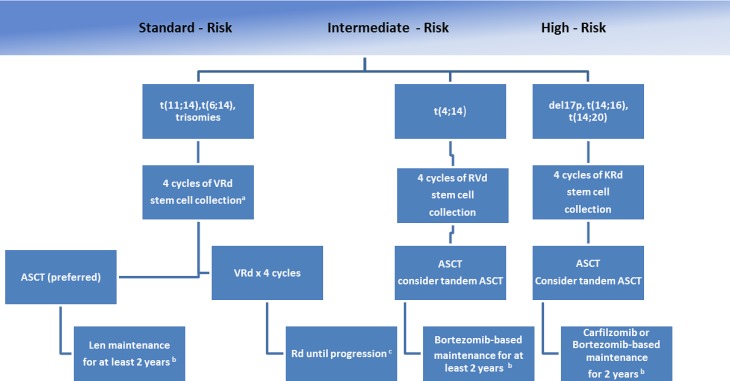
The treatment of newly diagnosed multiple myeloma has changed dramatically over the past 20 years, from near uniform application of chemotherapy to a patient performance status- and risk-based approach. Furthermore, initiation of treatment criteria have evolved from a pure end-organ damage-based definition to include risk factors of transformation to frank myeloma. Besides, the mainly cytogenetically defined Multiple Myeloma (MM) risk status, transplant eligibility of patients still serves primarily to allocate patients within a rational treatment algorithm. While all transplant-eligible MM patients should receive a triplet induction therapy followed by autologous transplantation and, in most cases, lenalidomide maintenance, other therapeutic elements (e. g., other maintenance strategies, consolidation, tandem transplantation,..) have to be decided on an individualized appraisal of risk and toxicities. Standard-risk patients should never be undertreated, as they derive the highest relative benefit from using the best available registered therapies. However, high-risk patients should be preferentially treated inside clinical trials testing additive innovative treatments, as the improvement in the prognosis of this group of patients by standard therapies has been underwhelming. Furthermore, the evaluation process of non-transplant-eligible patients should always comprise an evaluation of performance status, frailty, and comorbidities (e. g., a comprehensive geriatric assessment) to facilitate the allocation of individualized therapies.
在过去20年中,新诊断多发性骨髓瘤的治疗发生了巨大变化,从几乎统一应用化疗转变为基于患者体能状态和风险的治疗方法。此外,治疗起始标准已从单纯基于终末器官损害的定义演变为包括转化为明显骨髓瘤的风险因素。此外,除了主要通过细胞遗传学定义的多发性骨髓瘤(MM)风险状态外,患者的移植资格在合理的治疗方案中仍主要用于分配患者。虽然所有适合移植的MM患者都应接受三联诱导治疗,随后进行自体移植,并且在大多数情况下接受来那度胺维持治疗,但其他治疗要素(例如,其他维持策略、巩固治疗、串联移植等)必须根据对风险和毒性的个体化评估来决定。标准风险患者绝不应接受不足的治疗,因为他们从使用最佳可用的注册疗法中获得的相对益处最大。然而,高危患者应优先在测试附加创新疗法的临床试验中接受治疗,因为标准疗法对这组患者预后的改善并不显著。此外,对不适合移植的患者进行评估时,应始终包括对体能状态、虚弱程度和合并症(例如,全面的老年评估)的评估,以促进个体化治疗的分配。