Weatherhead PET Center, Division of Cardiology, Department of Medicine, McGovern Medical School at UTHealth and Memorial Hermann Hospital, Houston, TX, USA.
Department of Cardiology, Catharina Hospital, Eindhoven, Netherlands.
Eur Heart J. 2018 Jul 21;39(28):2646-2655. doi: 10.1093/eurheartj/ehy126.
Echocardiography and tomographic imaging have documented dynamic changes in aortic stenosis (AS) geometry and severity during both the cardiac cycle and stress-induced increases in cardiac output. However, corresponding pressure gradient vs. flow relationships have not been described.
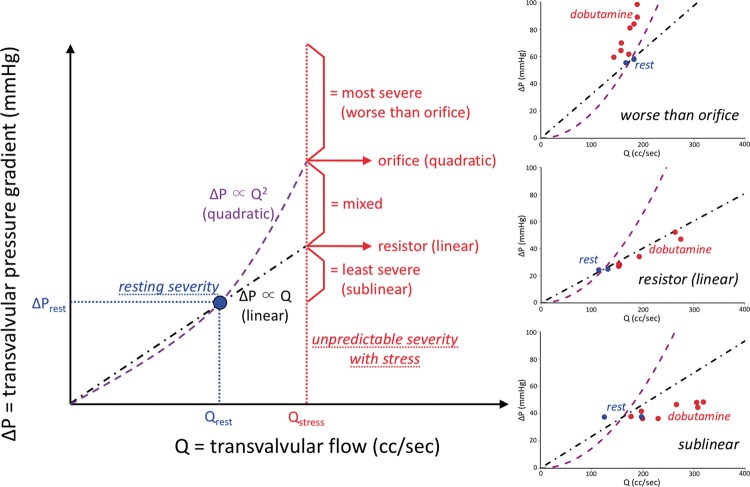
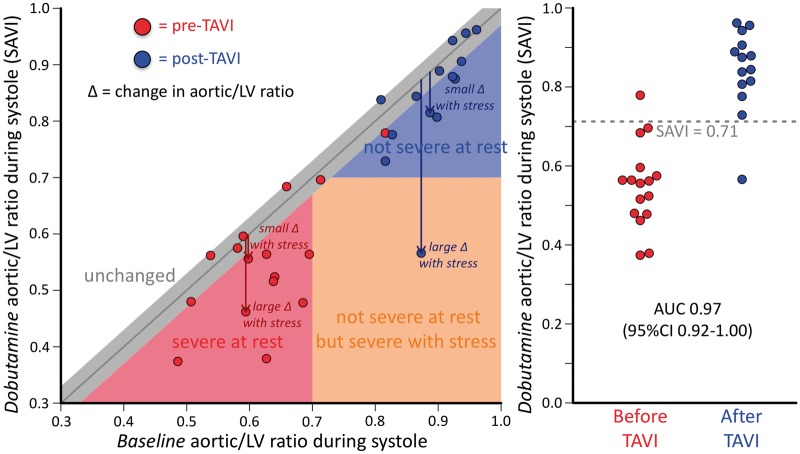
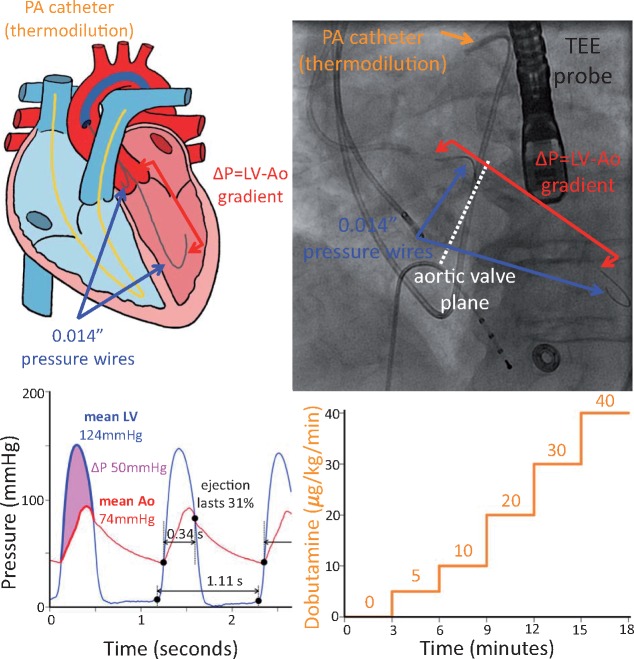
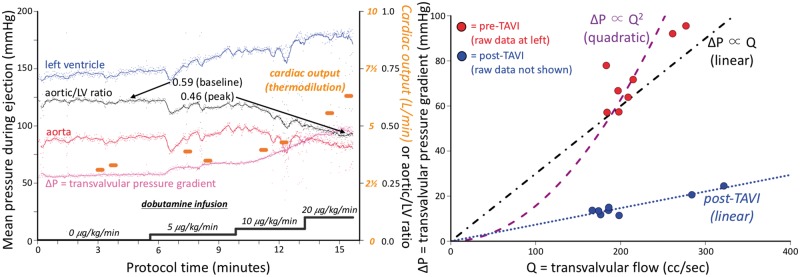
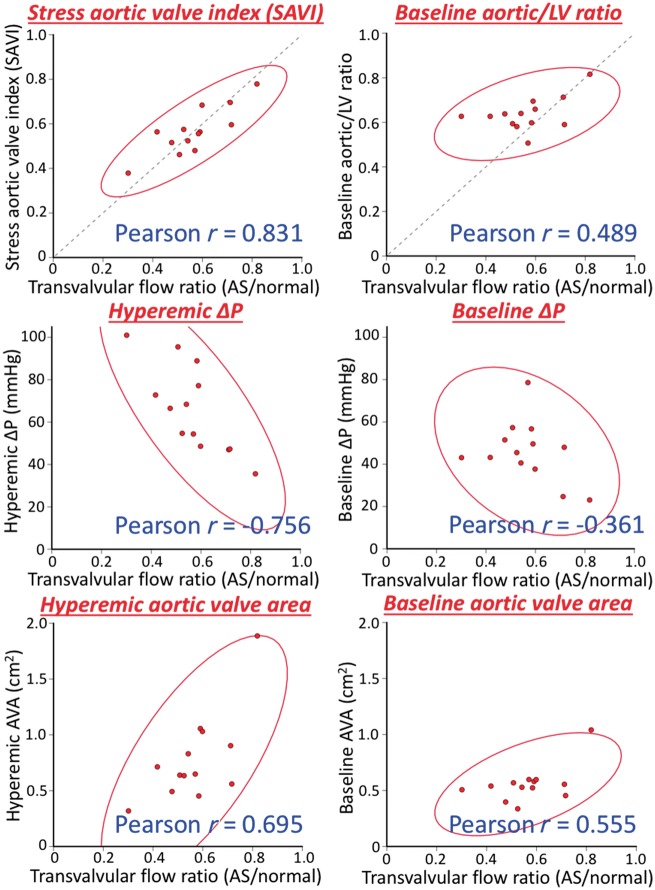
We recruited 16 routine transcatheter aortic valve implantations (TAVI's) for graded dobutamine infusions both before and after implantation; 0.014″ pressure wires in the aorta and left ventricle (LV) continuously measured the transvalvular pressure gradient (ΔP) while a pulmonary artery catheter regularly assessed cardiac output by thermodilution. Before TAVI, ΔP did not display a consistent relationship with transvalvular flow (Q). Neither linear resistor (median R2 0.16) nor quadratic orifice (median R2 < 0.01) models at rest predicted stress observations; the severely stenotic valve behaved like a combination. The unitless ratio of aortic to left ventricular pressures during systolic ejection under stress conditions correlated best with post-TAVI flow improvement. After TAVI, a highly linear relationship (median R2 0.96) indicated a valid valve resistance.
Pressure loss vs. flow curves offer a fundamental fluid dynamic synthesis for describing aortic valve pathophysiology. Severe AS does not consistently behave like an orifice (as suggested by Gorlin) or a resistor, whereas TAVI devices behave like a pure resistor. During peak dobutamine, the ratio of aortic to left ventricular pressures during systolic ejection provides a 'fractional flow reserve' of the aortic valve that closely approximates the complex, changing fluid dynamics. Because resting assessment cannot reliably predict stress haemodynamics, 'valvular fractional flow' warrants study to explain exertional symptoms in patients with only moderate AS at rest.
超声心动图和断层成像技术已经记录了在心动周期和心输出量应激增加期间主动脉瓣狭窄(AS)几何形状和严重程度的动态变化。然而,相应的压力梯度与流量关系尚未描述。
我们招募了 16 例行经导管主动脉瓣植入术(TAVI)的患者,在植入前后进行分级多巴酚丁胺输注;主动脉和左心室(LV)中的 0.014″压力线连续测量跨瓣压力梯度(ΔP),而肺动脉导管通过热稀释法定期评估心输出量。在 TAVI 之前,ΔP 与跨瓣流量(Q)之间没有一致的关系。无论是线性电阻器(中位数 R2 为 0.16)还是二次孔口(中位数 R2<0.01)模型在休息时都不能预测应激观察结果;严重狭窄的瓣膜表现为两者的结合。在应激条件下,收缩期射血期间主动脉与左心室压力的无单位比值与 TAVI 后流量改善相关性最好。TAVI 后,高度线性关系(中位数 R2 为 0.96)表明有效瓣膜阻力。
压力损失与流量曲线为描述主动脉瓣病理生理学提供了基本的流体动力学综合。严重 AS 并不像 Gorlin 所建议的那样始终表现为孔口(或阻力器),而 TAVI 装置则表现为纯阻力器。在多巴酚丁胺峰值期间,收缩期射血期间主动脉与左心室压力的比值提供了主动脉瓣的“分数流量储备”,该比值非常接近复杂且不断变化的流体动力学。由于静息评估不能可靠地预测应激血液动力学,因此“瓣膜分数流量”值得研究,以解释在静息时仅患有中度 AS 的患者的运动症状。