Department of Radiation Oncology, Aichi Cancer Center Hospital, Chikusa-ku, Nagoya, Japan.
Department of Radiology, Aichi Medical University Hospital, Yazako-Karimata, Nagakute, Aichi, 480-1195, Japan.
Radiat Oncol. 2018 Apr 4;13(1):62. doi: 10.1186/s13014-018-1012-3.
Intensity-modulated radiotherapy is useful for cervical oesophageal carcinoma (CEC); however, increasing low-dose exposure to the lung may lead to radiation pneumonitis. Nevertheless, an irradiation technique that avoids the lungs has never been examined due to the high difficulty of dose optimization. In this study, we examined the efficacy of helical tomotherapy that can restrict beamlets passing virtual blocks during dose optimization computing (block plan) in reducing the lung dose.
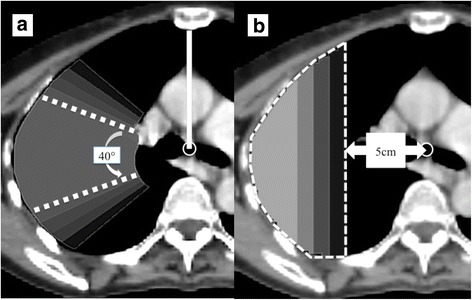
Fifteen patients with CEC were analysed. The primary/nodal lesion and prophylactic nodal region with adequate margins were defined as the planning target volume (PTV)-60 Gy and PTV-48 Gy, respectively. Nineteen plans per patient were made and compared (total: 285 plans), including non-block and block plans with several shapes and sizes.
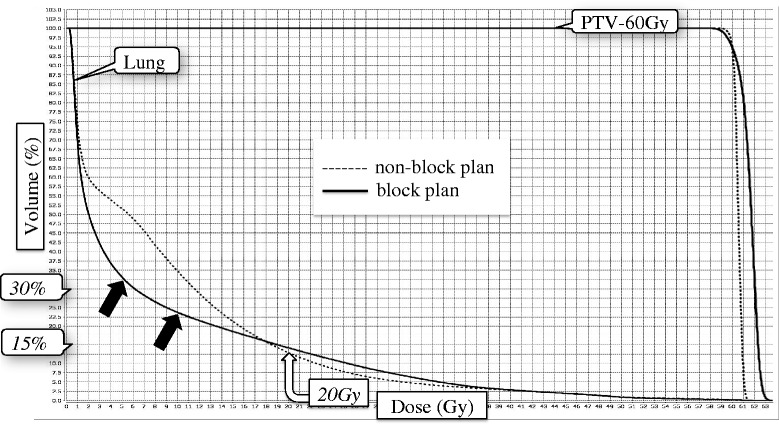
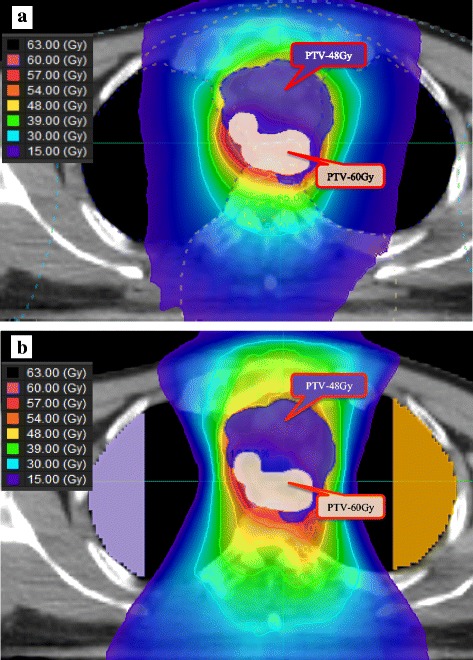
The most appropriate block model was semi-circular, 8 cm outside of the tracheal bifurcation, with a significantly lower lung dose compared to that of non-block plans; the mean lung volumes receiving 5 Gy, 10 Gy, 20 Gy, and the mean lung dose were 31.3% vs. 48.0% (p < 0.001), 22.4% vs. 39.4% (p < 0.001), 13.2% vs. 16.0% (p = 0.028), and 7.1 Gy vs. 9.6 Gy (p < 0.001), respectively. Both the block and non-block plans were comparable in terms of the homogeneity and conformity indexes of PTV-60 Gy: 0.05 vs. 0.04 (p = 0.100) and 0.82 vs. 0.85 (p = 0.616), respectively. The maximum dose of the spinal cord planning risk volume increased slightly (49.4 Gy vs. 47.9 Gy, p = 0.002). There was no significant difference in the mean doses to the heart and the thyroid gland. Prolongation of the delivery time was less than 1 min (5.6 min vs. 4.9 min, p = 0.010).
The block plan for CEC could significantly reduce the lung dose, with acceptable increment in the spinal dose and a slightly prolonged delivery time.
调强放疗对颈段食管癌(CEC)有效;然而,增加肺部的低剂量照射可能导致放射性肺炎。然而,由于剂量优化的难度很高,从未检查过避免肺部照射的照射技术。在这项研究中,我们检查了螺旋断层放疗的疗效,该技术可以在剂量优化计算(块计划)期间限制通过虚拟块的射束,从而降低肺部剂量。
分析了 15 例 CEC 患者。将原发/淋巴结病变和预防性淋巴结区域与足够的边界定义为计划靶区(PTV)-60Gy 和 PTV-48Gy。每位患者制定了 19 个计划,并进行了比较(总计:285 个计划),包括非块和块计划,具有几种形状和大小。
最合适的块模型为半圆形,位于气管分叉外 8cm 处,与非块计划相比,肺剂量显著降低;肺 5Gy、10Gy、20Gy 体积平均值分别为 31.3%和 48.0%(p<0.001)、22.4%和 39.4%(p<0.001)、13.2%和 16.0%(p=0.028)、7.1Gy 和 9.6Gy(p<0.001);PTV-60Gy 的均匀性和适形性指数在块和非块计划中相似:0.05 与 0.04(p=0.100)和 0.82 与 0.85(p=0.616);脊髓计划风险体积的最大剂量略有增加(49.4Gy 和 47.9Gy,p=0.002);心脏和甲状腺的平均剂量无显著差异。输送时间的延长小于 1 分钟(5.6 分钟与 4.9 分钟,p=0.010)。
CEC 的块计划可以显著降低肺部剂量,同时脊髓剂量略有增加,输送时间略有延长。