Abdo Joe, Cornell David L, Mittal Sumeet K, Agrawal Devendra K
Department of Clinical and Translational Science, Creighton University School of Medicine, Omaha, NE, United States.
Department of Surgery, CHI Health Creighton University Medical Center, Omaha, NE, United States.
Front Oncol. 2018 Mar 28;8:85. doi: 10.3389/fonc.2018.00085. eCollection 2018.
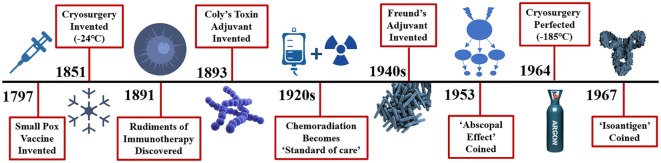
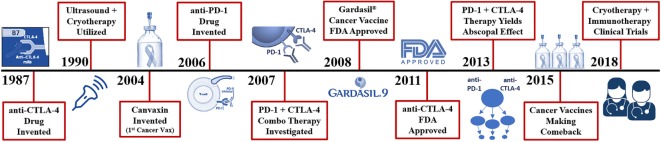
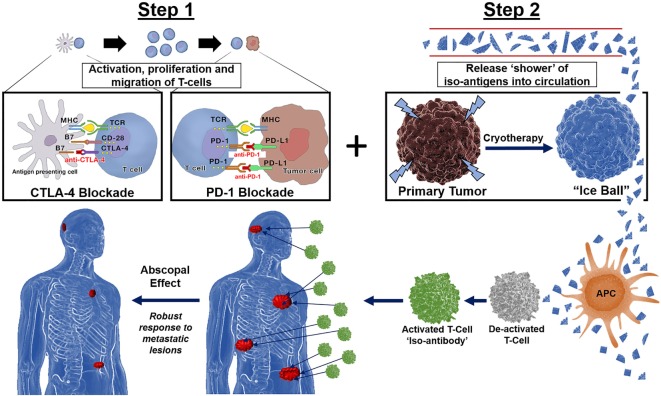
Since the 1920s the gold standard for treating cancer has been surgery, which is typically preceded or followed with chemotherapy and/or radiation, a process that perhaps contributes to the destruction of a patient's immune defense system. Cryosurgery ablation of a solid tumor is mechanistically similar to a vaccination where hundreds of unique antigens from a heterogeneous population of tumor cells derived from the invading cancer are released. However, releasing tumor-derived self-antigens into circulation may not be sufficient enough to overcome the checkpoint escape mechanisms some cancers have evolved to avoid immune responses. The potentiated immune response caused by blocking tumor checkpoints designed to prevent programmed cell death may be the optimal treatment method for the immune system to recognize these new circulating cryoablated self-antigens. Preclinical and clinical evidence exists for the complementary roles for Cytotoxic T-lymphocyte-associated protein (CTLA-4) and PD-1 antagonists in regulating adaptive immunity, demonstrating that combination immunotherapy followed by cryosurgery provides a more targeted immune response to distant lesions, a phenomenon known as the abscopal effect. We propose that when the host's immune system has been "primed" with combined anti-CTLA-4 and anti-PD-1 adjuvants prior to cryosurgery, the preserved cryoablated tumor antigens will be presented and processed by the host's immune system resulting in a robust cytotoxic CD8 T-cell response. Based on recent investigations and well-described biochemical mechanisms presented herein, a polyvalent autoinoculation of many tumor-specific antigens, derived from a heterogeneous population of tumor cancer cells, would present to an unhindered yet pre-sensitized immune system yielding a superior advantage in locating, recognizing, and destroying tumor cells throughout the body.
自20世纪20年代以来,治疗癌症的金标准一直是手术,通常在手术前后进行化疗和/或放疗,这一过程可能会导致患者免疫防御系统遭到破坏。实体瘤的冷冻消融手术在机制上类似于接种疫苗,会释放出数百种来自侵袭性癌症的异质性肿瘤细胞群体中的独特抗原。然而,将肿瘤衍生的自身抗原释放到循环系统中可能不足以克服某些癌症为避免免疫反应而进化出的检查点逃逸机制。通过阻断旨在防止程序性细胞死亡的肿瘤检查点所引发的增强免疫反应,可能是免疫系统识别这些新的循环冷冻消融自身抗原的最佳治疗方法。细胞毒性T淋巴细胞相关蛋白(CTLA-4)和PD-1拮抗剂在调节适应性免疫方面具有互补作用,这一点已有临床前和临床证据,表明冷冻手术后进行联合免疫疗法能对远处病变产生更具针对性的免疫反应,即所谓的远隔效应。我们提出,在冷冻手术前用抗CTLA-4和抗PD-1佐剂联合“激活”宿主免疫系统,保留的冷冻消融肿瘤抗原将由宿主免疫系统呈递和处理,从而产生强大的细胞毒性CD8 T细胞反应。基于最近的研究以及本文所述的详细生化机制,来自异质性肿瘤癌细胞群体的多种肿瘤特异性抗原进行多价自体接种,将呈递给未受阻碍但已预先致敏的免疫系统,在定位、识别和摧毁全身肿瘤细胞方面具有显著优势。