Department of Pediatrics, The Children's Hospital of Philadelphia, Philadelphia, PA; Department of Biostatistics, Epidemiology, and Informatics, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
Am J Kidney Dis. 2018 Jun;71(6):783-792. doi: 10.1053/j.ajkd.2017.12.011. Epub 2018 Apr 10.
RATIONALE & OBJECTIVE: The KDIGO (Kidney Disease: Improving Global Outcomes) guideline for chronic kidney disease (CKD) presented an international classification system that ranks patients' risk for CKD progression. Few data for children informed guideline development.
Observational cohort study.
SETTINGS & PARTICIPANTS: Children aged 1 to 18 years enrolled in the North American Chronic Kidney Disease in Children (CKiD) cohort study and the European Effect of Strict Blood Pressure Control and ACE Inhibition on the Progression of CRF in Pediatric Patients (ESCAPE) trial.
Level of estimated glomerular filtration rate (eGFR) and proteinuria (urine protein-creatinine ratio [UPCR]) at study entry.
A composite event of renal replacement therapy, 50% reduction in eGFR, or eGFR<15mL/min/1.73m. eGFR was estimated using the CKiD-derived "bedside" equation.
Accelerated failure time models of the composite outcome using a conventional generalized gamma distribution. Likelihood ratio statistics of nested models were used to amalgamate levels of similar risk.
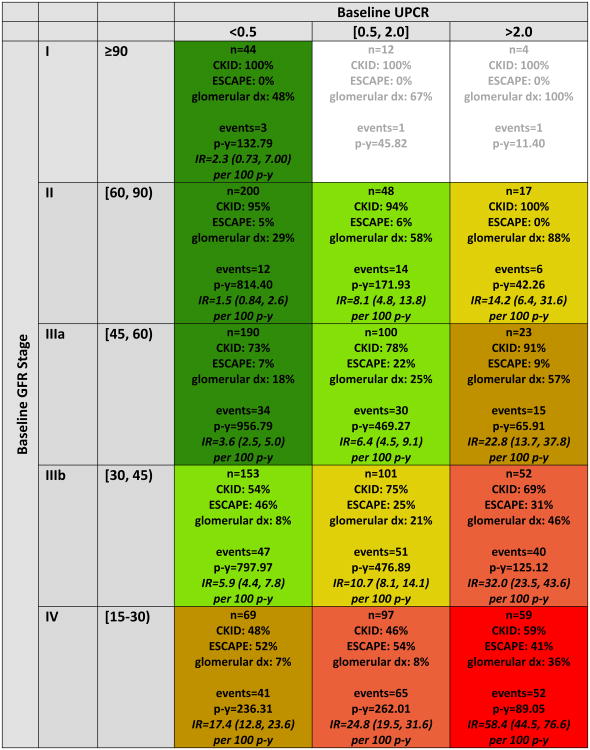
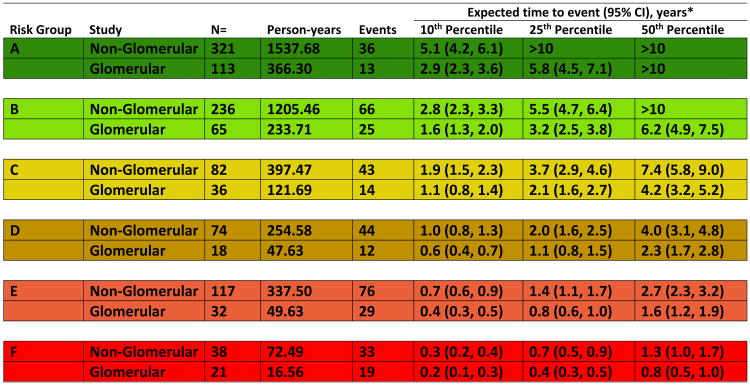
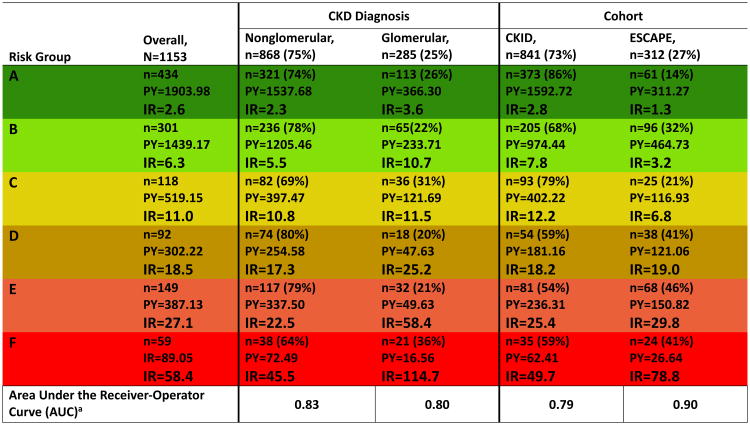
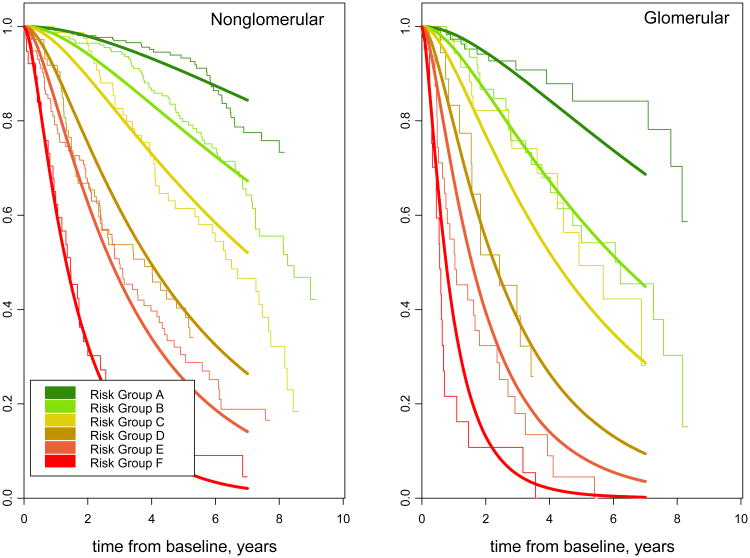
Among 1,232 children, median age was 12 (IQR, 8-15) years, median eGFR was 47 (IQR, 33-62) mL/min/1.73m, 60% were males, and 13% had UPCRs>2.0mg/mg at study entry. 6 ordered stages with varying combinations of eGFR categories (60-89, 45-59, 30-44, and 15-29mL/min/1.73m) and UPCR categories (<0.5, 0.5-2.0, and >2.0mg/mg) described the risk continuum. Median times to event ranged from longer than 10 years for eGFRs of 45 to 90mL/min/1.73m and UPCRs<0.5mg/mg to 0.8 years for eGFRs of 15 to 30mL/min/1.73m and UPCRs>2mg/mg. Children with glomerular disease were estimated to have a 43% shorter time to event than children with nonglomerular disease. Cross-validation demonstrated risk patterns that were consistent across the 10 subsample validation models.
Observational study, used cross-validation rather than external validation.
CKD staged by level of eGFR and proteinuria characterizes the timeline of progression and can guide management strategies in children.
KDIGO(肾脏疾病:改善全球预后)慢性肾脏病(CKD)指南提出了一种国际分类系统,对 CKD 进展风险进行患者分层。该指南的制定过程中,儿童相关数据较少。
观察性队列研究。
年龄为 1 至 18 岁的儿童,纳入北美慢性肾脏病儿童队列研究(CKiD)和儿童患者严格血压控制和 ACE 抑制对 CRF 进展的影响(ESCAPE)试验。
研究入组时估计肾小球滤过率(eGFR)和蛋白尿(尿蛋白与肌酐比值[UPCR])水平。
肾脏替代治疗、eGFR 下降 50%或 eGFR<15mL/min/1.73m 复合终点事件。eGFR 使用 CKiD 衍生的“床边”方程进行估算。
使用常规广义伽马分布对复合结局进行加速失效时间模型分析。使用嵌套模型的似然比统计数据对风险相似水平进行合并。
在 1232 名儿童中,中位年龄为 12(IQR,8-15)岁,中位 eGFR 为 47(IQR,33-62)mL/min/1.73m,60%为男性,13%在研究入组时 UPCR>2.0mg/mg。6 个有序阶段,eGFR 类别(60-89、45-59、30-44 和 15-29mL/min/1.73m)和 UPCR 类别(<0.5、0.5-2.0 和>2.0mg/mg)有不同的组合,描述了风险连续体。事件中位时间从 eGFR 为 45 至 90mL/min/1.73m 和 UPCR<0.5mg/mg 的 10 年以上到 eGFR 为 15 至 30mL/min/1.73m 和 UPCR>2mg/mg 的 0.8 年不等。与非肾小球疾病儿童相比,肾小球疾病儿童的事件中位时间估计缩短了 43%。交叉验证表明,10 个样本验证模型的风险模式一致。
观察性研究,使用交叉验证而不是外部验证。
根据 eGFR 和蛋白尿水平对 CKD 进行分期,可描述进展的时间线,并指导儿童管理策略。