Brigham and Women's Hospital Heart & Vascular Center, Harvard Medical School, Boston, Massachusetts; Richard and Susan Smith Center for Outcomes Research in Cardiology, Division of Cardiology, Beth Israel Deaconess Medical and Harvard Medical School, Boston, Massachusetts.
Washington University School of Medicine, Saint Louis, Missouri.
JACC Heart Fail. 2018 May;6(5):379-387. doi: 10.1016/j.jchf.2017.11.010. Epub 2018 Apr 11.
The purpose of this study was to examine the association of 30-day payments for an episode of heart failure (HF) care at the hospital level with patient outcomes.
There is increased focus among policymakers on improving value for HF care, given its rising prevalence and associated financial burden in the United States; however, little is known about the relationship between payments and mortality for a 30-day episode of HF care.
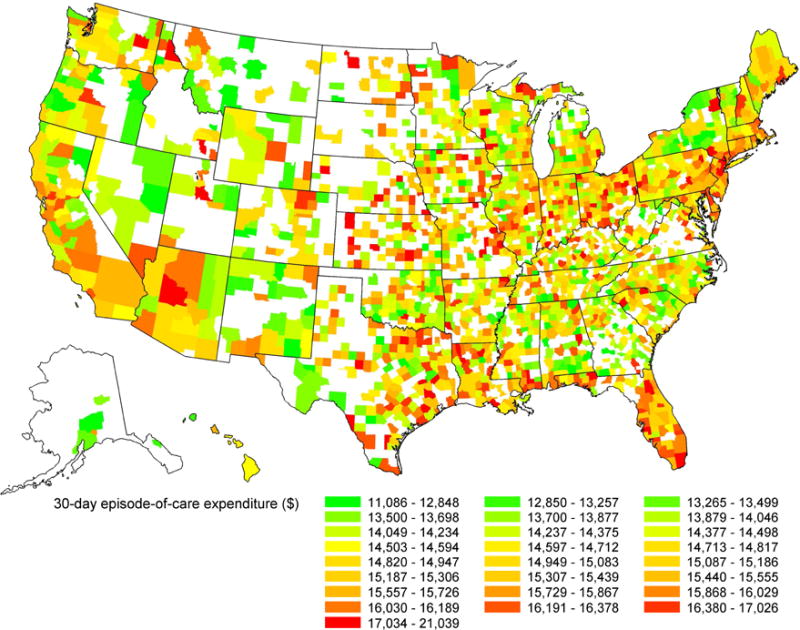
Using Medicare claims data for all fee-for-service beneficiaries hospitalized for HF between July 1, 2011, and June 30, 2014, we examined the association between 30-day Medicare payments at the hospital level (beginning with a hospital admission for HF and across multiple settings following discharge) and patient 30-day mortality using mixed-effect logistic regression models.
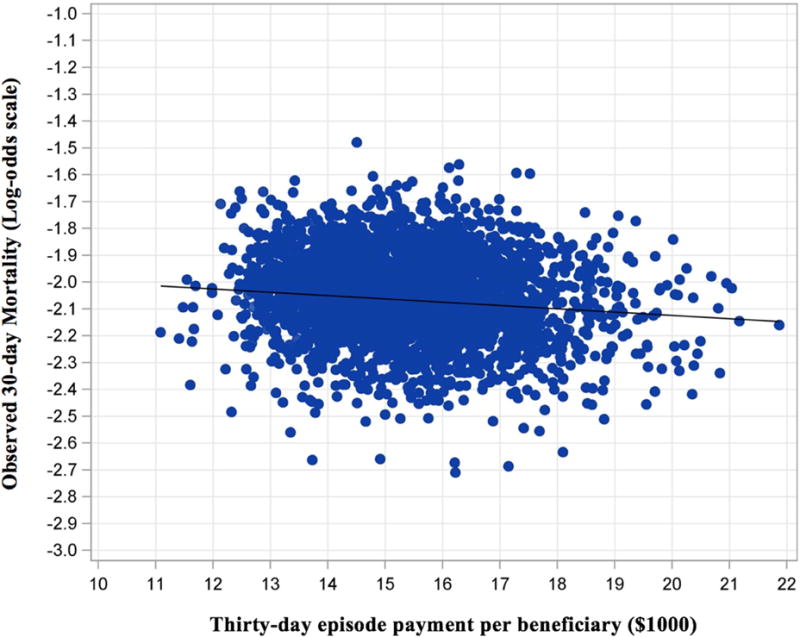
We included 1,343,792 patients hospitalized for HF across 2,948 hospitals. Mean hospital-level 30-day Medicare payments per beneficiary were $15,423 ± $1,523. Overall observed mortality in the cohort was 11.3%. Higher hospital-level 30-day payments were associated with lower patient mortality after adjustment for patient characteristics (odds ratio per $1,000 increase in payments: 0.961; 95% confidence interval [CI]: 0.954 to 0.967). This relationship was slightly attenuated after accounting for hospital characteristics and HF volume, but remained significant (odds ratio per $1,000 increase: 0.968; 95% CI: 0.962 to 0.975). Additional adjustment for potential mediating factors, including cardiac service capability and post-acute service use, did not significantly affect the relationship.
Higher hospital-level 30-day episode payments were associated with lower patient mortality following a hospitalization for HF. This has implications for policies that incentivize reduction in payments without considering value. Further investigation is needed to understand the mechanisms that underlie this relationship.
本研究旨在探讨医院层面心力衰竭(HF)治疗 30 天内支付情况与患者结局之间的关系。
鉴于 HF 在全美患病率不断上升且相关经济负担沉重,政策制定者日益关注改善 HF 治疗的价值;然而,对于 HF 30 天治疗期内支付情况与死亡率之间的关系,人们知之甚少。
利用 2011 年 7 月 1 日至 2014 年 6 月 30 日期间所有接受 HF 治疗的按服务收费受益人的医疗保险索赔数据,我们使用混合效应逻辑回归模型,考察了医院层面(从 HF 入院开始,出院后在多个场所)30 天内医疗保险支付情况与患者 30 天死亡率之间的关系。
我们纳入了 2948 家医院的 1343792 名 HF 住院患者。每位受益人的平均医院层面 30 天内医疗保险支付额为 15423 美元±1523 美元。该队列中总体观察到的死亡率为 11.3%。调整患者特征后,较高的医院层面 30 天支付额与患者死亡率降低相关(每增加 1000 美元支付额,比值比:0.961;95%置信区间[CI]:0.954 至 0.967)。在考虑到医院特征和 HF 量后,这种关系略有减弱,但仍具有统计学意义(每增加 1000 美元支付额,比值比:0.968;95%CI:0.962 至 0.975)。进一步调整潜在的中介因素,包括心脏服务能力和急性期后服务使用情况,并未显著影响该关系。
HF 住院治疗后,较高的医院层面 30 天治疗期内支付额与患者死亡率降低相关。这对那些不考虑价值而激励降低支付额的政策具有启示意义。需要进一步研究以了解这种关系的潜在机制。