Chamberlain Ronald S, Sond Jaswinder, Mahendraraj Krishnaraj, Lau Christine Sm, Siracuse Brianna L
Department of Surgery, Saint Barnabas Medical Center, Livingston.
Department of Surgery, Rutgers New Jersey Medical School, Rutgers University, Newark, NJ, USA.
Int J Gen Med. 2018 Apr 9;11:127-141. doi: 10.2147/IJGM.S150676. eCollection 2018.
Chronic heart failure (CHF), which affects >5 million Americans, accounts for >1 million hospitalizations annually. As a part of the Hospital Readmission Reduction Program, the Affordable Care Act requires that the Centers for Medicare and Medicaid Services reduce payments to hospitals with excess readmissions. This study sought to develop a scale that reliably predicts readmission rates among patients with CHF.
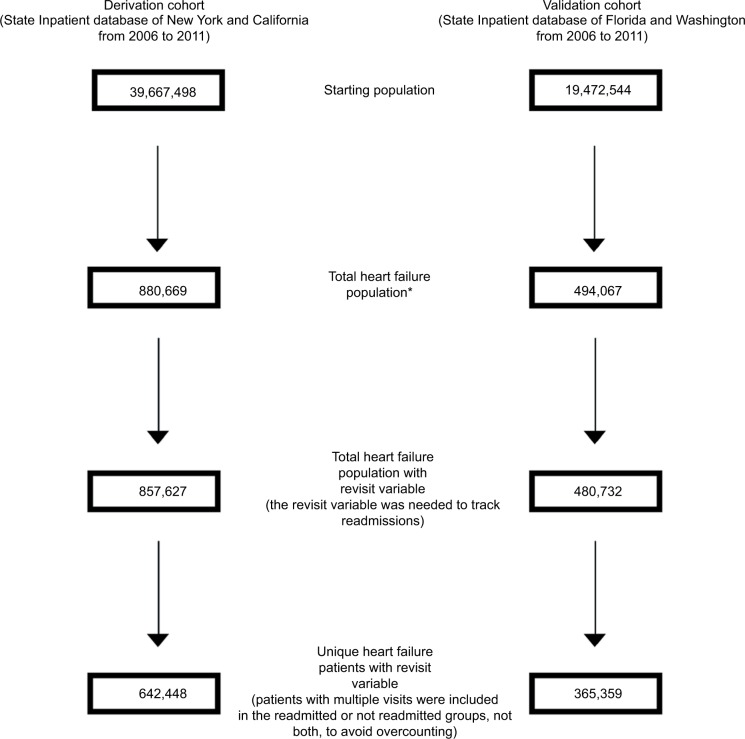
The State Inpatient Database (2006-2011) was utilized, and discharge data including demographic and clinical characteristics on 642,448 patients with CHF from California and New York (derivation cohort) and 365,359 patients with CHF from Florida and Washington (validation cohort) were extracted. The Readmission After Heart Failure (RAHF) scale was developed to predict readmission risk.
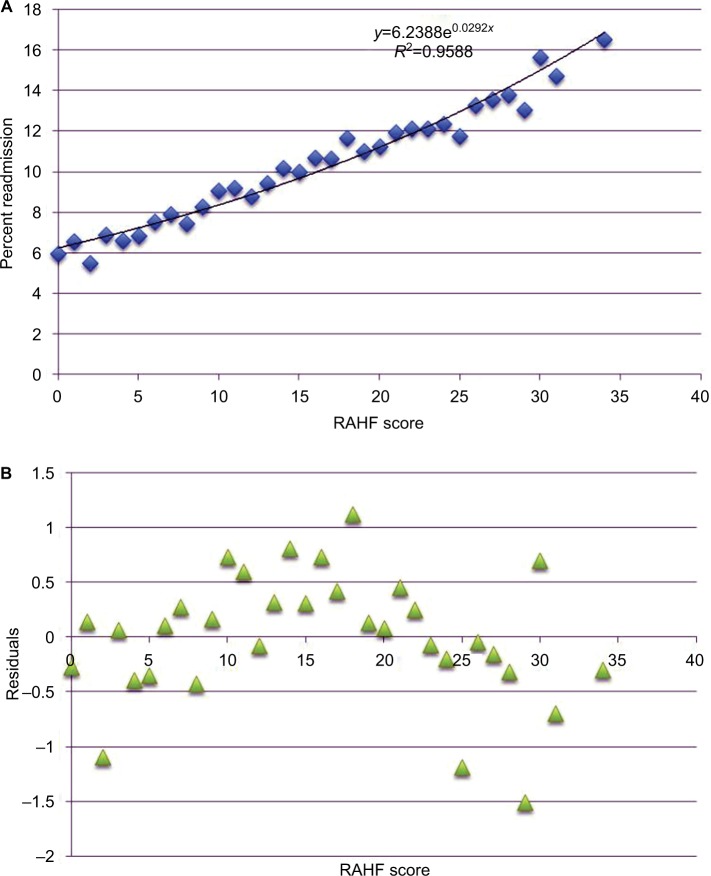
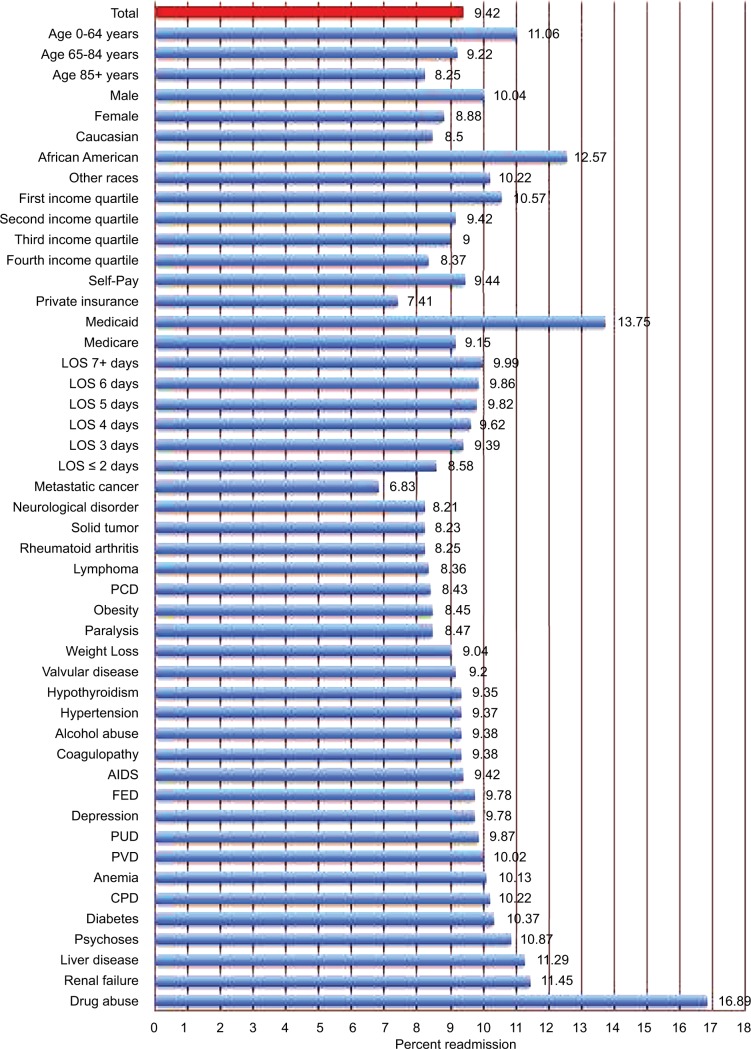
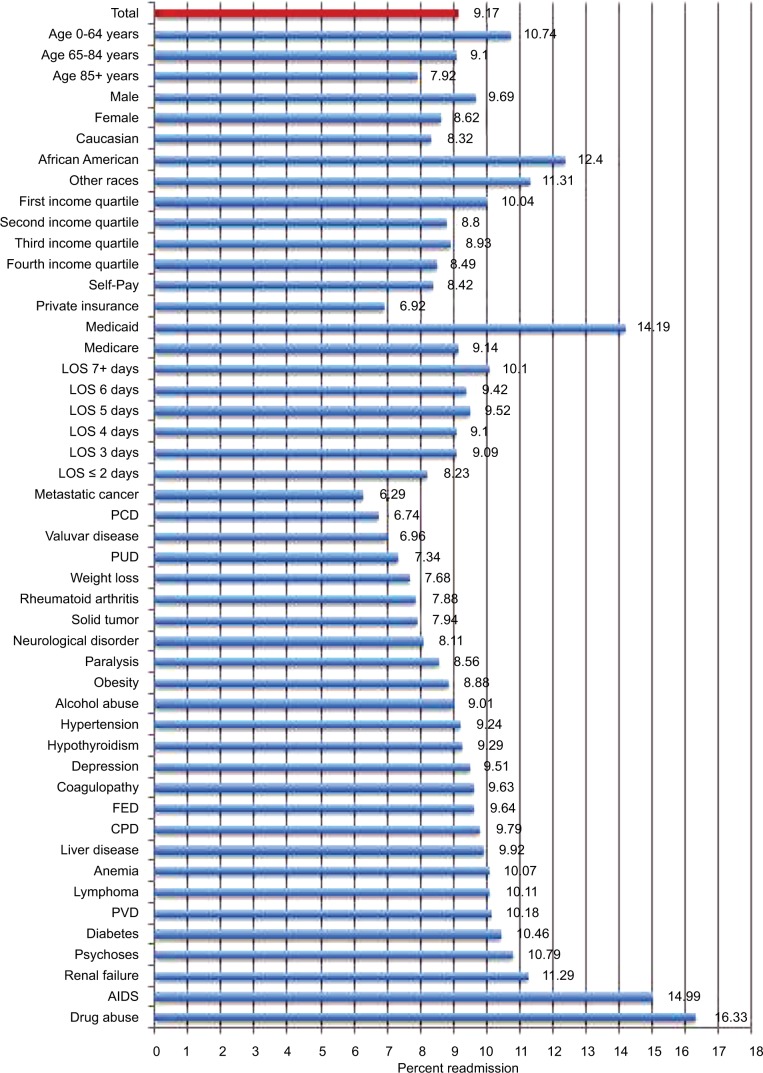
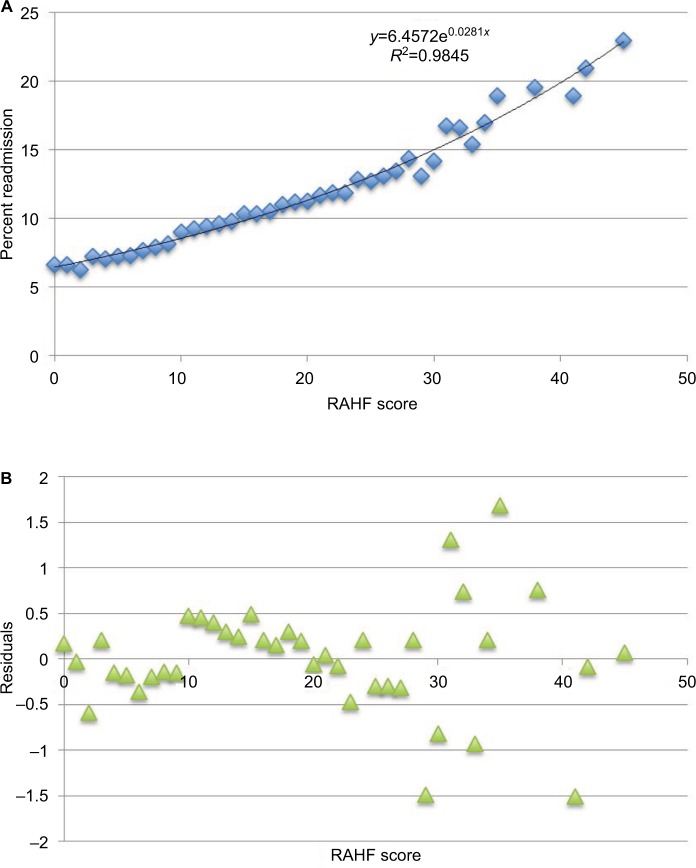
The 30-day readmission rates were 9.42 and 9.17% (derivation and validation cohorts, respectively). Age <65 years, male gender, first income quartile, African American race, race other than African American or Caucasian, Medicare, Medicaid, self-pay/no insurance, drug abuse, renal failure, chronic pulmonary disorder, diabetes, depression, and fluid and electrolyte disorder were associated with higher readmission risk after hospitalization for CHF. The RAHF scale was created and explained the 95% of readmission variability within the validation cohort. The RAHF scale was then used to define the following three levels of risk for readmission: low (RAHF score <12; 7.58% readmission rate), moderate (RAHF score 12-15; 9.78% readmission rate), and high (RAHF score >15; 12.04% readmission rate). The relative risk of readmission was 1.67 for the high-risk group compared with the low-risk group.
The RAHF scale reliably predicts a patient's 30-day CHF readmission risk based on demographic and clinical factors present upon initial admission. By risk-stratifying patients, using models such as the RAHF scale, strategies tailored to each patient can be implemented to improve patient outcomes and reduce health care costs.
慢性心力衰竭(CHF)影响着超过500万美国人,每年导致超过100万人住院治疗。作为《降低医院再入院率计划》的一部分,《平价医疗法案》要求医疗保险和医疗补助服务中心减少对再入院率过高的医院的支付。本研究旨在开发一种能够可靠预测CHF患者再入院率的量表。
利用州住院数据库(2006 - 2011年),提取了来自加利福尼亚州和纽约州的642,448例CHF患者(推导队列)以及来自佛罗里达州和华盛顿州的365,359例CHF患者(验证队列)的出院数据,包括人口统计学和临床特征。开发了心力衰竭后再入院(RAHF)量表以预测再入院风险。
30天再入院率分别为9.42%和9.17%(推导队列和验证队列)。年龄<65岁、男性、收入处于第一四分位数、非裔美国人种族、非裔美国人或白种人以外的种族、医疗保险、医疗补助、自费/无保险、药物滥用、肾衰竭、慢性肺部疾病、糖尿病、抑郁症以及液体和电解质紊乱与CHF住院后的再入院风险较高相关。创建了RAHF量表,该量表解释了验证队列中95%的再入院变异性。然后使用RAHF量表定义以下三个再入院风险级别:低风险(RAHF评分<12;再入院率7.58%)、中度风险(RAHF评分12 - 15;再入院率9.78%)和高风险(RAHF评分>15;再入院率12.04%)。与低风险组相比,高风险组的再入院相对风险为1.67。
RAHF量表基于初次入院时存在的人口统计学和临床因素可靠地预测患者30天CHF再入院风险。通过使用RAHF量表等模型对患者进行风险分层,可以实施针对每个患者的策略,以改善患者预后并降低医疗成本。