Bolkenstein H E, Draaisma W A, van de Wall Bjm, Consten Ecj, Broeders Iamj
Department of Surgery, Meander Medical Centre, 3800 BM, Amersfoort, The Netherlands.
Robotics and Mechatronics, Faculty of Electrical Engineering, University of Twente, 7500 AE, Enschede, The Netherlands.
Int J Colorectal Dis. 2018 Jul;33(7):863-869. doi: 10.1007/s00384-018-3055-1. Epub 2018 Apr 21.
Conservative treatment strategy without antibiotics in patients with uncomplicated diverticulitis (UD) has proven to be safe. The aim of the current study is to assess the clinical course of UD patients who were initially treated without antibiotics and to identify risk factors for treatment failure.
A retrospective cohort study was performed including all patients with a CT-proven episode of UD (defined as modified Hinchey 1A). Only non-immunocompromised patients who presented without signs of sepsis were included. Patients that received antibiotics within 24 h after or 2 weeks prior to presentation were excluded from analysis. Patient characteristics, clinical signs, and laboratory parameters were collected. Treatment failure was defined as (re)admittance, mortality, complications (perforation, abscess, colonic obstruction, urinary tract infection, pneumonia) or need for antibiotics, operative intervention, or percutaneous abscess drainage within 30 days after initial presentation. Multivariable logistic regression analyses were used to quantify which variables are independently related to treatment failure.
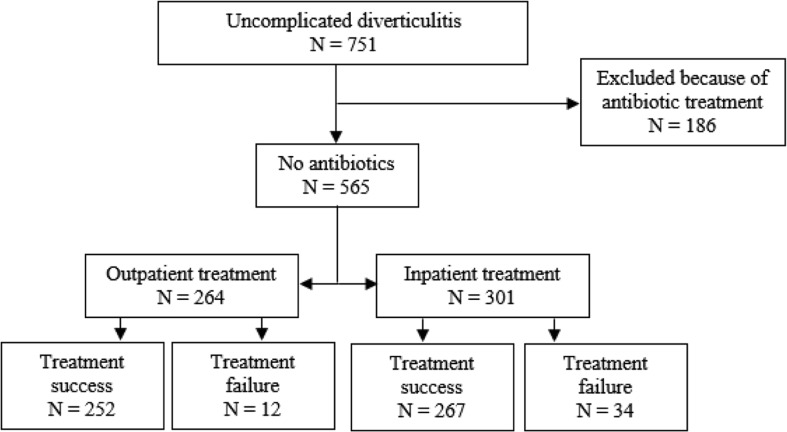
Between January 2005 and January 2017, 751 patients presented at the emergency department with a CT-proven UD. Of these, 186 (25%) patients were excluded from analysis because of antibiotic treatment. A total of 565 patients with UD were included. Forty-six (8%) patients experienced treatment failure. In the multivariable analysis, a high CRP level (> 170 mg/L) was a significant predictive factor for treatment failure.
UD patients with a CRP level > 170 mg/L are at higher risk for non-antibiotic treatment failure. Clinical physicians should take this finding in consideration when selecting patients for non-antibiotic treatment.
已证实,在无并发症的憩室炎(UD)患者中,不使用抗生素的保守治疗策略是安全的。本研究的目的是评估最初未使用抗生素治疗的UD患者的临床病程,并确定治疗失败的危险因素。
进行了一项回顾性队列研究,纳入所有经CT证实为UD发作(定义为改良Hinchey 1A)的患者。仅纳入无败血症迹象的非免疫功能低下患者。在就诊后24小时内或就诊前2周内接受抗生素治疗的患者被排除在分析之外。收集患者特征、临床体征和实验室参数。治疗失败定义为在初次就诊后30天内再次入院、死亡、出现并发症(穿孔、脓肿、结肠梗阻、尿路感染、肺炎)或需要使用抗生素、进行手术干预或经皮脓肿引流。采用多变量逻辑回归分析来量化哪些变量与治疗失败独立相关。
2005年1月至2017年1月期间,751例患者因CT证实为UD而到急诊科就诊。其中,186例(25%)患者因接受抗生素治疗而被排除在分析之外。总共纳入了565例UD患者。46例(8%)患者出现治疗失败。在多变量分析中,高CRP水平(>170mg/L)是治疗失败的一个重要预测因素。
CRP水平>170mg/L的UD患者非抗生素治疗失败的风险较高。临床医生在选择非抗生素治疗的患者时应考虑这一发现。