Department of Radiation Oncology, Erasmus MC Cancer Institute, Groene Hilledijk 301, 3075, EA, Rotterdam, The Netherlands.
Universitätsmedizin Mannheim, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany.
Radiat Oncol. 2018 Apr 23;13(1):74. doi: 10.1186/s13014-018-1032-z.
Postoperative/adjuvant radiotherapy of advanced gastric cancer involves a large planning target volume (PTV) with multi-concave shapes which presents a challenge for volumetric modulated arc therapy (VMAT) planning. This study investigates the advantages of automated VMAT planning for this site compared to manual VMAT planning by expert planners.
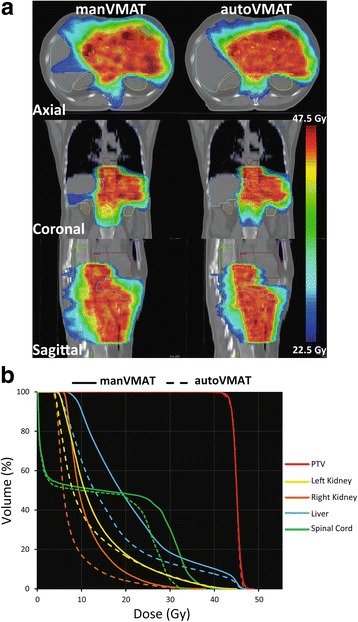
For 20 gastric cancer patients in the postoperative/adjuvant setting, dual-arc VMAT plans were generated using fully automated multi-criterial treatment planning (autoVMAT), and compared to manually generated VMAT plans (manVMAT). Both automated and manual plans were created to deliver a median dose of 45 Gy to the PTV using identical planning and segmentation parameters. Plans were evaluated by two expert radiation oncologists for clinical acceptability. AutoVMAT and manVMAT plans were also compared based on dose-volume histogram (DVH) and predicted normal tissue complication probability (NTCP) analysis.
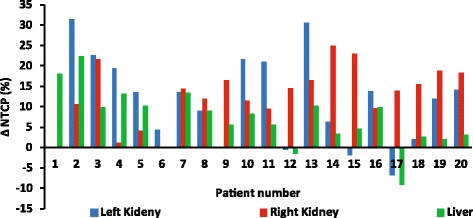
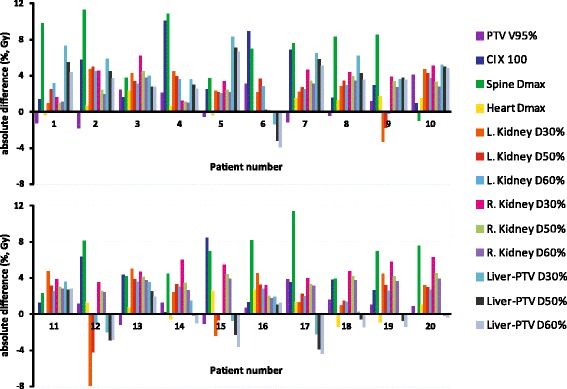
Both manVMAT and autoVMAT plans were considered clinically acceptable. Target coverage was similar (manVMAT: 96.6 ± 1.6%, autoVMAT: 97.4 ± 1.0%, p = 0.085). With autoVMAT, median kidney dose was reduced on average by > 25%; (for left kidney from 11.3 ± 2.1 Gy to 8.9 ± 3.5 Gy (p = 0.002); for right kidney from 9.2 ± 2.2 Gy to 6.1 ± 1.3 Gy (p < 0.001)). Median dose to the liver was lower as well (18.8 ± 2.3 Gy vs. 17.1 ± 3.6 Gy, p = 0.048). In addition, Dmax of the spinal cord was significantly reduced (38.3 ± 3.7 Gy vs. 31.6 ± 2.6 Gy, p < 0.001). Substantial improvements in dose conformity and integral dose were achieved with autoVMAT plans (4.2% and 9.1%, respectively; p < 0.001). Due to the better OAR sparing in the autoVMAT plans compared to manVMAT plans, the predicted NTCPs for the left and right kidney and the liver-PTV were significantly reduced by 11.3%, 12.8%, 7%, respectively (p ≤ 0.001). Delivery time and total number of monitor units were increased in autoVMAT plans (from 168 ± 19 s to 207 ± 26 s, p = 0.006) and (from 781 ± 168 MU to 1001 ± 134 MU, p = 0.003), respectively.
For postoperative/adjuvant radiotherapy of advanced gastric cancer, involving a complex target shape, automated VMAT planning is feasible and can substantially reduce the dose to the kidneys and the liver, without compromising the target dose delivery.
晚期胃癌术后/辅助放疗涉及多凹形的大计划靶区(PTV),这对容积调强弧形治疗(VMAT)计划提出了挑战。本研究旨在通过专家规划师评估自动 VMAT 计划与手动 VMAT 计划相比,在该部位的优势。
对于 20 例胃癌术后/辅助放疗患者,采用全自动多标准治疗计划(autoVMAT)生成双弧 VMAT 计划,并与手动生成的 VMAT 计划(manVMAT)进行比较。使用相同的计划和分割参数,为 PTV 生成中位数剂量为 45 Gy 的计划。由两位资深放射肿瘤学家对临床可接受性进行评估。根据剂量-体积直方图(DVH)和预测正常组织并发症概率(NTCP)分析,对 autoVMAT 和 manVMAT 计划进行比较。
manVMAT 和 autoVMAT 计划均被认为是临床可接受的。靶区覆盖率相似(manVMAT:96.6 ± 1.6%,autoVMAT:97.4 ± 1.0%,p = 0.085)。使用 autoVMAT,中位数肾脏剂量平均降低> 25%;(左侧肾脏从 11.3 ± 2.1 Gy 降至 8.9 ± 3.5 Gy(p = 0.002);右侧肾脏从 9.2 ± 2.2 Gy 降至 6.1 ± 1.3 Gy(p < 0.001))。肝脏的中位数剂量也较低(18.8 ± 2.3 Gy 比 17.1 ± 3.6 Gy,p = 0.048)。此外,脊髓的 Dmax 明显降低(38.3 ± 3.7 Gy 比 31.6 ± 2.6 Gy,p < 0.001)。自动 VMAT 计划可显著提高剂量适形性和积分剂量(分别为 4.2%和 9.1%,p < 0.001)。由于与 manVMAT 计划相比,autoVMAT 计划对 OAR 的保护更好,左肾、右肾和肝-PTV 的预测 NTCP 分别显著降低了 11.3%、12.8%、7%(p ≤ 0.001)。自动 VMAT 计划的治疗时间和总监视器单位数分别增加(从 168 ± 19 s 增加到 207 ± 26 s,p = 0.006)和(从 781 ± 168 MU 增加到 1001 ± 134 MU,p = 0.003)。
对于涉及复杂靶形的晚期胃癌术后/辅助放疗,自动 VMAT 计划是可行的,可以显著降低肾脏和肝脏的剂量,同时不影响靶区剂量分布。