Carter John B, Carter Sara, Saschenbrecker Sandra, Goeckeritz Bruce E
Lexington Medical Center, West Columbia, SC, United States.
Institute for Experimental Immunology, Euroimmun AG, Luebeck, Germany.
Front Med (Lausanne). 2018 Apr 9;5:88. doi: 10.3389/fmed.2018.00088. eCollection 2018.
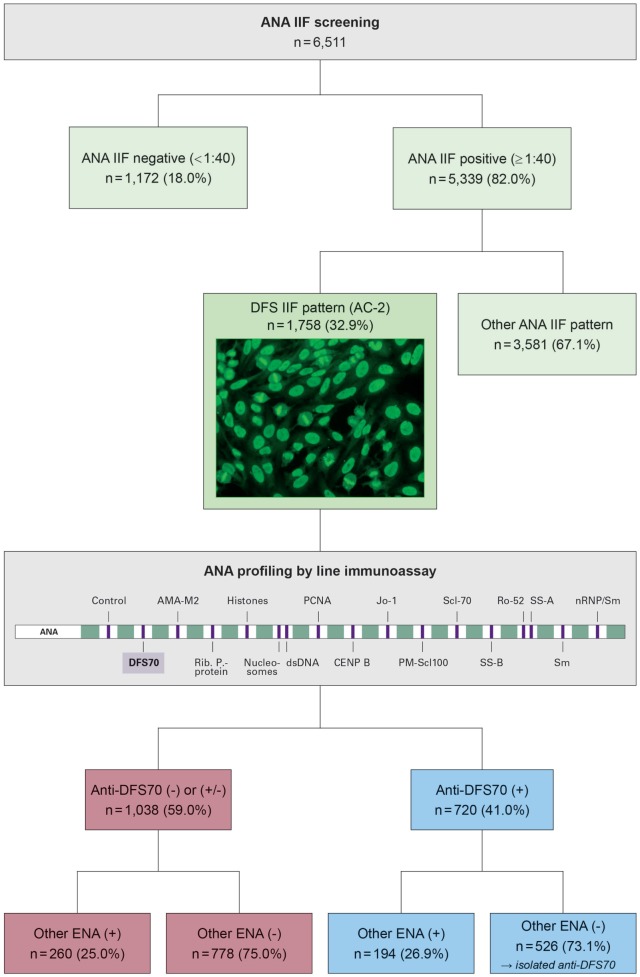
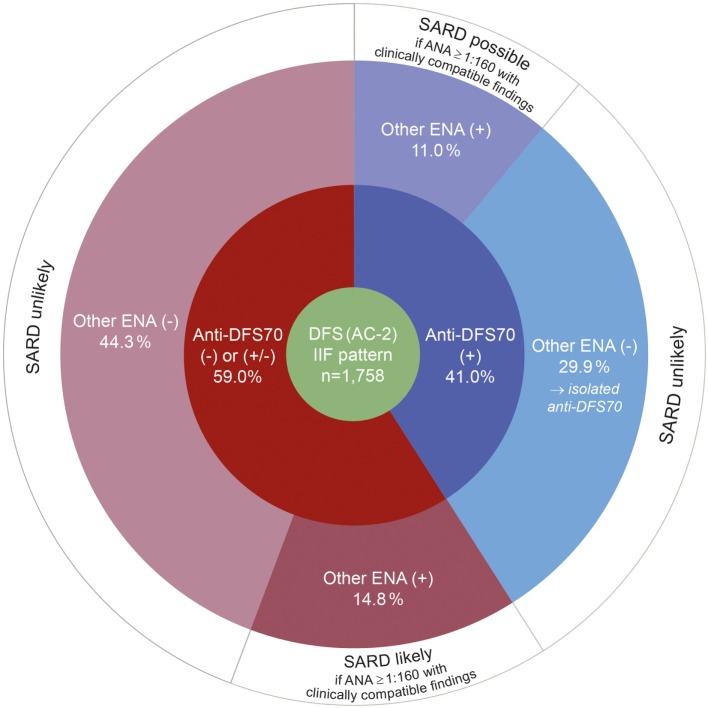
Antinuclear autoantibodies (ANA) displaying a dense fine speckled pattern (DFS, ICAP AC-2) on HEp-2 cells are frequently observed in clinical laboratory referrals, often associated with anti-DFS70 specificity. Anti-DFS70 positive patients rarely develop systemic autoimmune rheumatic disease (SARD), especially in the absence of clinical evidence or additional anti-extractable nuclear antigen (ENA) antibodies, prompting suggestions that an isolated DFS70-specific ENA may be an exclusionary finding for SARD. In this study, the frequency and diagnostic significance of anti-DFS70 autoantibodies was investigated in a community hospital cohort of patients undergoing routine ANA testing. ANA screening was performed by HEp-20-10-based indirect immunofluorescence, followed by ENA profiling using a multiparametric line immunoassay (LIA). Of 6,511 patient samples tested for ANA in 2016, the DFS pattern was identified in 1,758 (27.0%), 720 (41.0%) of which were anti-DFS70 positive by LIA. Of these, 526 (73.1%) revealed isolated anti-DFS70 reactivity, while 194 (26.9%) showed additional ENA specificities. Among 1,038 anti-DFS70 negative or borderline samples, 778 (75.0%) were ENA profile negative, while the remaining 260 (25.0%) showed a varied presence of other ENA specificities. Chart reviews of patients with an isolated anti-DFS70 ANA affirmed that ANA-related SARD is rare in the absence of clinical evidence or other ENA specificities, there being no case thus far identified. Rheumatoid arthritis patients occasionally had an isolated anti-DFS70 ANA and were positive for rheumatoid factor and anti-cyclic citrullinated peptide antibodies. In conclusion, the recognition of a DFS ANA pattern using a mitotic-rich HEp-2 substrate, followed by confirmation of anti-DFS70 specificity should be a routine ANA testing service. Use of an expanded ENA profile and clinical correlation is necessary to affirm the "isolation" of anti-DFS70 as the cause of an ANA. Recognition of isolated anti-DFS70 ANA enables reassurance of patients that SARD is unlikely, thus avoiding referral for more extensive testing. The presence of significant elevations of other ENAs may reflect SARD and warrants close clinical correlation and follow-up.
在临床实验室送检样本中,经常观察到抗核自身抗体(ANA)在人喉表皮癌细胞(HEp-2)上呈现致密细颗粒型(DFS,ICAP AC-2),通常与抗DFS70特异性相关。抗DFS70阳性患者很少发生系统性自身免疫性风湿病(SARD),尤其是在缺乏临床证据或其他抗可提取核抗原(ENA)抗体的情况下,这提示孤立的DFS70特异性ENA可能是SARD的排除性发现。在本研究中,我们在一家社区医院对接受常规ANA检测的患者队列中,调查了抗DFS70自身抗体的频率及诊断意义。ANA筛查采用基于HEp-20-10的间接免疫荧光法进行,随后使用多参数线性免疫分析(LIA)进行ENA谱分析。在2016年检测ANA的6511份患者样本中,1758份(27.0%)呈现DFS模式,其中720份(41.0%)通过LIA检测为抗DFS70阳性。其中,526份(73.1%)显示孤立的抗DFS70反应性,而194份(26.9%)显示存在其他ENA特异性。在1038份抗DFS70阴性或临界样本中,778份(75.0%)ENA谱为阴性,其余260份(25.0%)显示存在不同的其他ENA特异性。对孤立抗DFS70 ANA患者的病历回顾证实,在缺乏临床证据或其他ENA特异性的情况下,ANA相关的SARD很少见,目前尚未发现此类病例。类风湿关节炎患者偶尔有孤立的抗DFS70 ANA,且类风湿因子和抗环瓜氨酸肽抗体呈阳性。总之,使用富含有丝分裂的HEp-2底物识别DFS ANA模式,随后确认抗DFS70特异性,应作为常规ANA检测服务。使用扩展的ENA谱并结合临床相关性,对于确认抗DFS70作为ANA病因的“孤立性”是必要的。识别孤立的抗DFS70 ANA可使患者放心,不太可能患有SARD,从而避免转诊进行更广泛的检测。其他ENA显著升高可能提示SARD,需要密切的临床相关性和随访。