Aston Medical Research Institute, Aston Medical School, Aston University, Aston Triangle, Birmingham, UK.
Centre for Cardiovascular Sciences, University of Birmingham, United Kingdom Queen Elizabeth Hospital, Metchley Drive, Birmingham, UK.
Europace. 2018 Nov 1;20(11):1804-1812. doi: 10.1093/europace/eux357.
There is a continuing debate as to whether cardiac resynchronization therapy-defibrillation (CRT-D) is superior to CRT-pacing (CRT-P), particularly in patients with non-ischaemic cardiomyopathy (NICM). We sought to quantify the clinical outcomes after primary prevention of CRT-D and CRT-P and identify whether these differed according to the aetiology of cardiomyopathy.
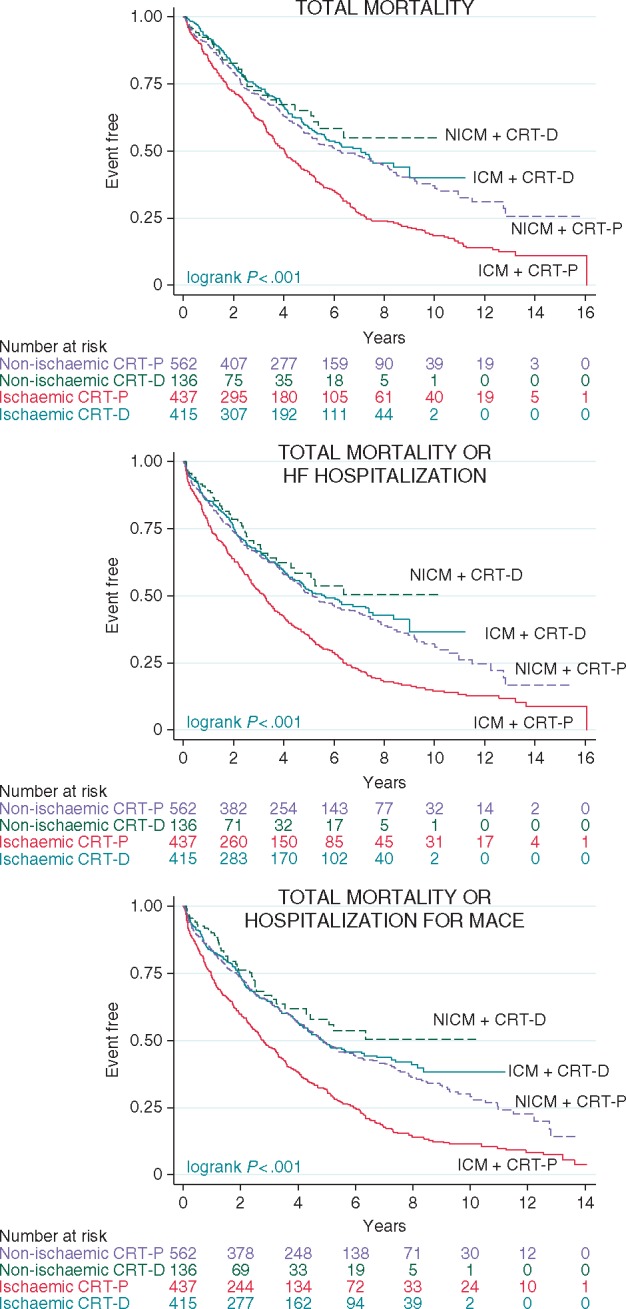
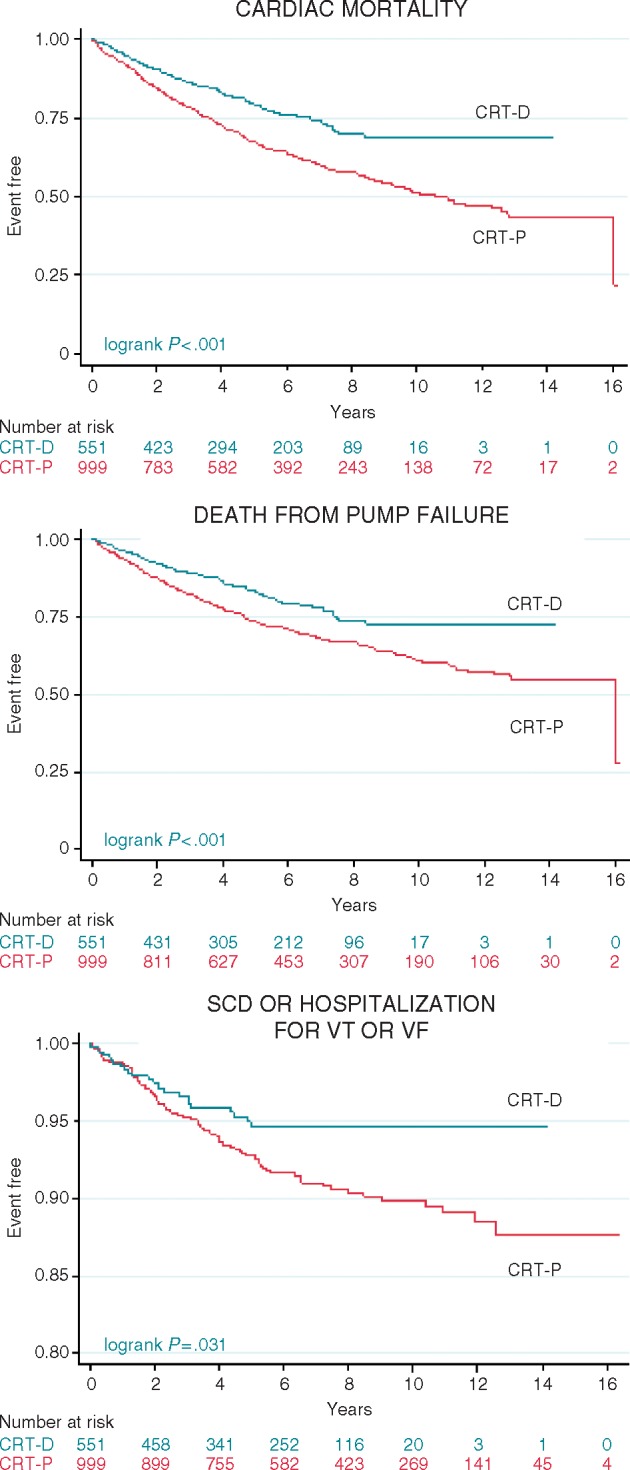
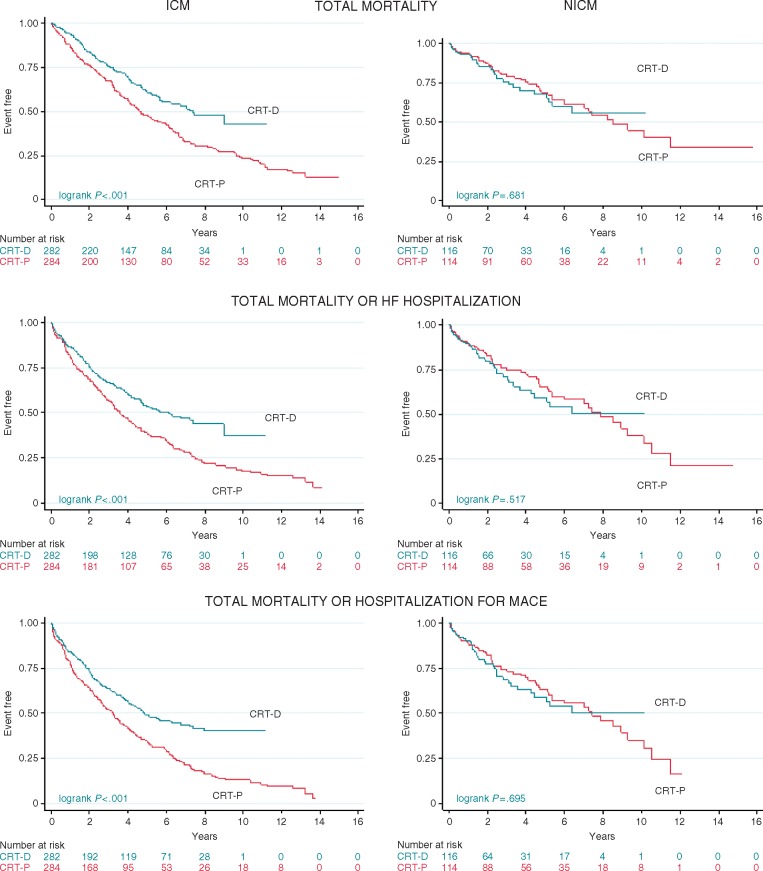
Analyses were undertaken in the total study population of patients treated with CRT-D (n = 551) or CRT-P (n = 999) and in propensity-matched samples. Device choice was governed by the clinical guidelines in the United Kingdom. In univariable analyses of the total study population, for a maximum follow-up of 16 years (median 4.7 years, interquartile range 2.4-7.1), CRT-D was associated with a lower total mortality [hazard ratio (HR) 0.72] and the composite endpoints of total mortality or heart failure (HF) hospitalization (HR 0.72) and total mortality or hospitalization for major adverse cardiac events (MACE; HR 0.71) (all P < 0.001). After propensity matching (n = 796), CRT-D was associated with a lower total mortality (HR 0.72) and the composite endpoints (all P < 0.01). When further stratified according to aetiology, CRT-D was associated with a lower total mortality (HR 0.62), total mortality or HF hospitalization (HR 0.63), and total mortality or hospitalization for MACE (HR 0.59) (all P < 0.001) in patients with ischaemic cardiomyopathy (ICM). There were no differences in outcomes between CRT-D and CRT-P in patients with NICM.
In this study of real-world clinical practice, CRT-D was superior to CRT-P with respect to total mortality and composite endpoints, independent of known confounders. The benefit of CRT-D was evident in ICM but not in NICM.
心脏再同步治疗除颤器(CRT-D)是否优于心脏再同步治疗起搏(CRT-P),特别是在非缺血性心肌病(NICM)患者中,一直存在争议。我们旨在量化 CRT-D 和 CRT-P 一级预防后的临床结局,并确定这些结局是否因心肌病的病因不同而有所不同。
在接受 CRT-D(n=551)或 CRT-P(n=999)治疗的患者的总研究人群以及倾向匹配样本中进行了分析。器械选择由英国的临床指南决定。在总研究人群的单变量分析中,对于最长 16 年的随访(中位数 4.7 年,四分位距 2.4-7.1),CRT-D 与总死亡率降低相关[风险比(HR)0.72]和总死亡率或心力衰竭(HF)住院的复合终点(HR 0.72)和总死亡率或主要不良心脏事件(MACE)住院的复合终点(HR 0.71)(均 P<0.001)。在倾向匹配后(n=796),CRT-D 与总死亡率降低相关(HR 0.72)和复合终点(均 P<0.01)。当根据病因进一步分层时,CRT-D 与总死亡率降低相关(HR 0.62)、总死亡率或 HF 住院的复合终点(HR 0.63)以及总死亡率或 MACE 住院的复合终点(HR 0.59)(均 P<0.001)在缺血性心肌病(ICM)患者中。在 NICM 患者中,CRT-D 和 CRT-P 之间的结局没有差异。
在这项真实世界临床实践的研究中,CRT-D 在总死亡率和复合终点方面优于 CRT-P,独立于已知的混杂因素。CRT-D 的益处在 ICM 中是明显的,但在 NICM 中则不然。