Udeshika W A E, Herath H M M T B, Dassanayake S U B, Pahalagamage S P, Kulatunga Aruna
National Hospital, Colombo, Sri Lanka.
BMC Res Notes. 2018 Apr 27;11(1):262. doi: 10.1186/s13104-018-3375-9.
Pancreatic cysts are being diagnosed more frequently because of the increasing usage of imaging techniques. A pseudocyst with the major diameter of 10 cm is termed as a giant cyst. Asymptomatic pseudo-cysts up to 6 cm in diameter can be safely observed and monitored without intervention, but larger and symptomatic pseudocysts require intervention.
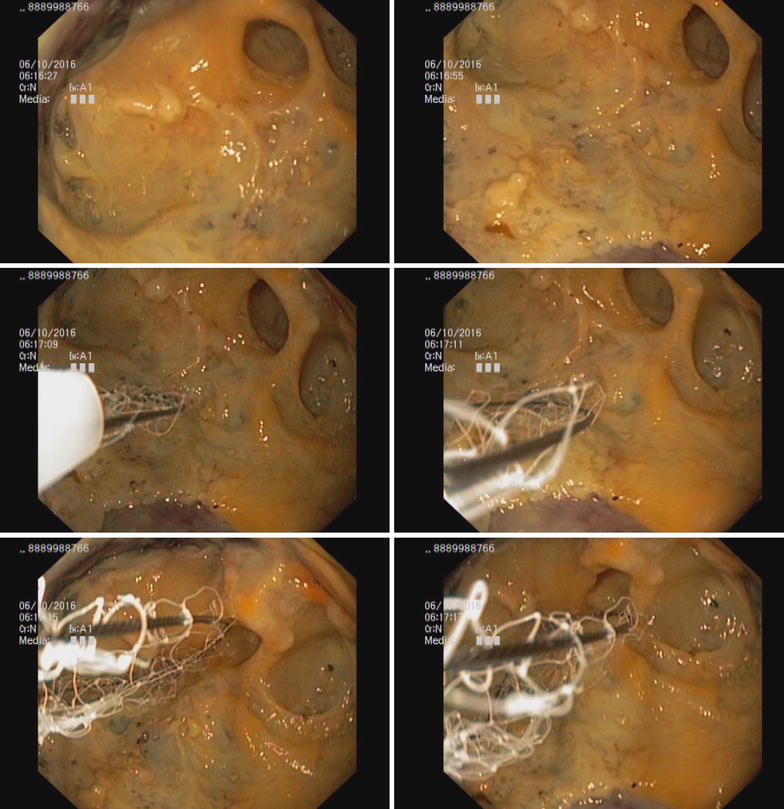
A 27-year-old Sri Lankan male, with history of heavy alcohol use, presented with progressive abdominal distension following an episode of acute pancreatitis. Contrast enhanced CT scan of the abdomen showed a large multilocular cystic lesion almost occupying the entire abdominal cavity and displacing the liver medially and the right dome of the diaphragm superiorly. The largest locule in the right side measured as 30 cm × 15 cm × 14 cm. Endoscopic ultrasound guided drainage of the cyst was performed. The cyst was entered into with an electrocautery-assisted cystotome and a lumen-opposing metal stent was deployed under fluoroscopic vision followed by dilatation with a 10 mm controlled radial expansion balloon. Repeat endoscopic ultrasound was done a week later due to persistence of the collection and a second stent was inserted. Then 10 French gauge × 10 cm double ended pigtails were inserted through both stents. The cysts were not visualized on subsequent Ultra sound scans. Stent removal was done after 3 weeks, leaving the pigtails insitu. The patient made an uneventful recovery.
Giant pancreatic pseudocysts are rare and earlier drainage is recommended before clinical deterioration. Some experts suggest that cystogastrostomy may not be appropriate for the treatment of giant pancreatic pseudocysts and in some instances external drainage of giant pancreatic pseudocysts may be safer than cystogastrostomy. Video-assisted pancreatic necrosectomy with internal drainage and laparoscopic cystogastrostomy were also tried with a good outcome. With our experience we suggest endoscopic guided internal drainage as a possible initial method of management of a giant pseudo cyst. However long-term follow up is needed with repeated imaging and endoscopy. In instances where the primary endoscopic internal drainage fails, surgical procedures may be required as a second line option.
由于成像技术的使用日益增加,胰腺囊肿的诊断越来越频繁。主要直径为10厘米的假性囊肿被称为巨大囊肿。直径达6厘米的无症状假性囊肿可在不进行干预的情况下安全观察和监测,但较大且有症状的假性囊肿需要干预。
一名27岁的斯里兰卡男性,有大量饮酒史,在一次急性胰腺炎发作后出现进行性腹胀。腹部增强CT扫描显示一个大的多房囊性病变,几乎占据整个腹腔,将肝脏向内推移,右膈穹窿向上移位。右侧最大的房腔尺寸为30厘米×15厘米×14厘米。对囊肿进行了内镜超声引导下引流。用电灼辅助囊肿切开刀进入囊肿,并在荧光透视下放置一个腔内对合金属支架,随后用10毫米可控径向扩张球囊进行扩张。由于积液持续存在,一周后再次进行内镜超声检查,并插入了第二个支架。然后通过两个支架插入10法式规格×10厘米的双猪尾导管。在随后的超声扫描中未发现囊肿。3周后取出支架,保留猪尾导管原位。患者顺利康复。
巨大胰腺假性囊肿罕见,建议在临床恶化前尽早引流。一些专家认为囊肿胃吻合术可能不适用于巨大胰腺假性囊肿的治疗,在某些情况下,巨大胰腺假性囊肿的外引流可能比囊肿胃吻合术更安全。也尝试了视频辅助胰腺坏死组织清除术加内引流和腹腔镜囊肿胃吻合术,效果良好。根据我们的经验,我们建议内镜引导下内引流作为巨大假性囊肿可能的初始治疗方法。然而,需要通过重复成像和内镜检查进行长期随访。在原发性内镜内引流失败的情况下,可能需要手术作为二线选择。