Cornelis F H, Martin M, Saut O, Buy X, Kind M, Palussiere J, Colin T
1University Bordeaux, IMB, UMR 5251; CNRS, IMB, UMR 5251; Bordeaux INP, IMB, UMR 5251, Talence, France.
2INRIA Bordeaux-sud-Ouest, team MONC, 200 Avenue de la Vieille Tour, 33405 Talence, France.
Eur Radiol Exp. 2017;1(1):16. doi: 10.1186/s41747-017-0015-4. Epub 2017 Oct 30.
Response evaluation criteria in solid tumours (RECIST) has significant limitations in terms of variability and reproducibility, which may not be independent. The aim of the study was to evaluate the precision of manual bi-dimensional segmentation of lung, liver metastases, and to quantify the uncertainty in tumour response assessment.
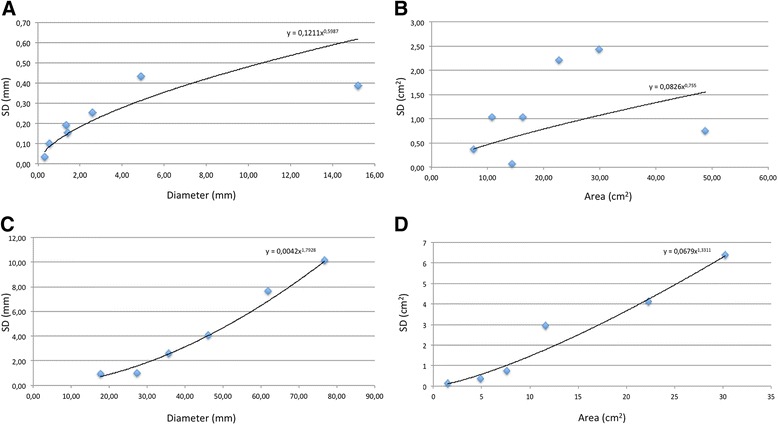
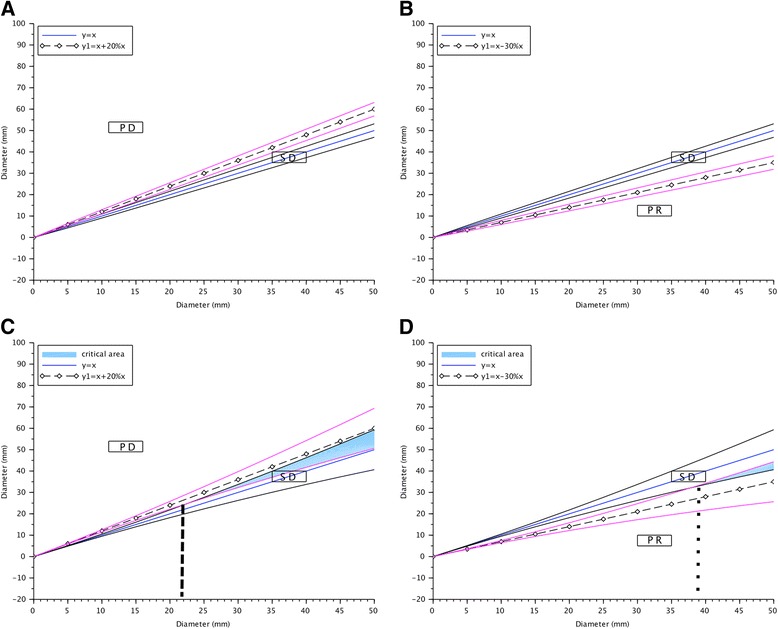
A total of 520 segmentations of metastases from six livers and seven lungs were independently performed by ten physicians and ten scientists on CT images, reflecting the variability encountered in clinical practice. Operators manually contoured the tumours, firstly independently according to the RECIST and secondly on a preselected slice. Diameters and areas were extracted from the segmentations. Mean standard deviations were used to build regression models and 95% confidence intervals (95% CI) were calculated for each tumour size and for limits of progressive disease (PD) and partial response (PR) derived from RECIST 1.1.
Thirteen aberrant segmentations (2.5%) were observed without significant differences between the physicians and scientists; only the mean area of liver tumours ( = 0.034) and mean diameter of lung tumours ( = 0.021) differed significantly. No difference was observed between the methods. Inter-observer agreement was excellent (intra-class correlation >0.90) for all variables. In liver, overlaps of the 95% CI with the 95% CI of limits of PD or PR were observed for diameters above 22.7 and 37.9 mm, respectively. An overlap of 95% CIs was systematically observed for area. No overlaps were observed in lung.
Although the experience of readers might not affect the precision of segmentation in lung and liver, the results of manual segmentation performed for tumour response assessment remain uncertain for large liver metastases.
实体瘤疗效评价标准(RECIST)在变异性和可重复性方面存在显著局限性,且二者可能并非相互独立。本研究旨在评估肺、肝转移瘤手动二维分割的精确性,并量化肿瘤反应评估中的不确定性。
10名医生和10名科研人员在CT图像上对来自6个肝脏和7个肺的转移瘤进行了总共520次分割,反映了临床实践中遇到的变异性。操作人员手动勾勒肿瘤轮廓,首先根据RECIST独立进行,其次在预选切片上进行。从分割结果中提取直径和面积。使用平均标准差建立回归模型,并针对每个肿瘤大小以及根据RECIST 1.1得出的疾病进展(PD)和部分缓解(PR)的界限计算95%置信区间(95%CI)。
观察到13次异常分割(2.5%),医生和科研人员之间无显著差异;仅肝肿瘤的平均面积(=0.034)和肺肿瘤的平均直径(=0.021)存在显著差异。两种方法之间未观察到差异。所有变量的观察者间一致性均极佳(组内相关>0.90)。在肝脏中,对于直径分别大于22.7和37.9mm的情况,观察到95%CI与PD或PR界限的95%CI存在重叠。对于面积,系统地观察到95%CI存在重叠。在肺中未观察到重叠。
尽管阅片者的经验可能不会影响肺和肝分割的精确性,但对于大的肝转移瘤,用于肿瘤反应评估的手动分割结果仍不确定。