Zhang Linlin, Terrando Niccolò, Xu Zhen-Zhong, Bang Sangsu, Jordt Sven-Eric, Maixner William, Serhan Charles N, Ji Ru-Rong
Department of Anesthesiology, Center for Translational Pain Medicine, Duke University Medical Center, Durham, NC, United States.
Department of Physiology, Center of Neuroscience, Key Laboratory of Medical Neurobiology of the Ministry of Health of China, Zhejiang University School of Medicine, Hangzhou, China.
Front Pharmacol. 2018 May 1;9:412. doi: 10.3389/fphar.2018.00412. eCollection 2018.
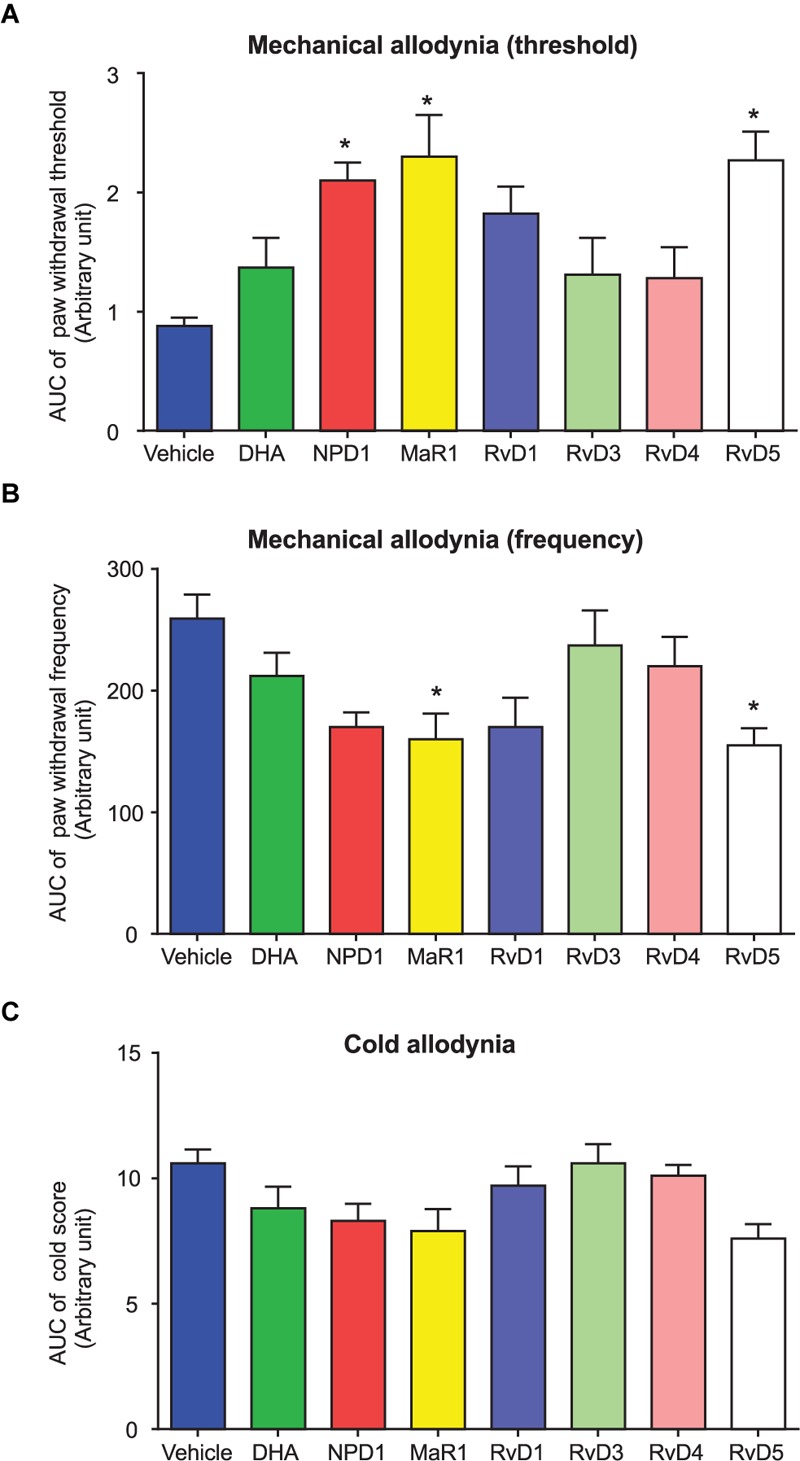
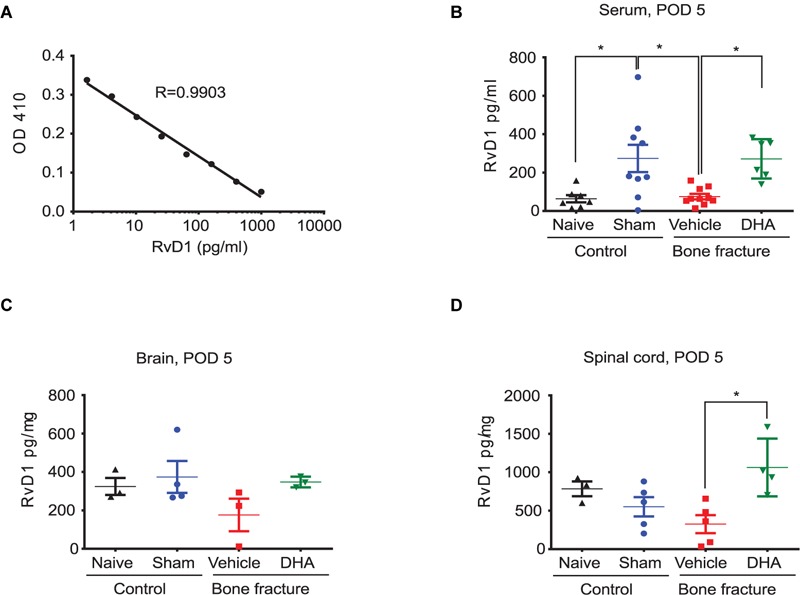
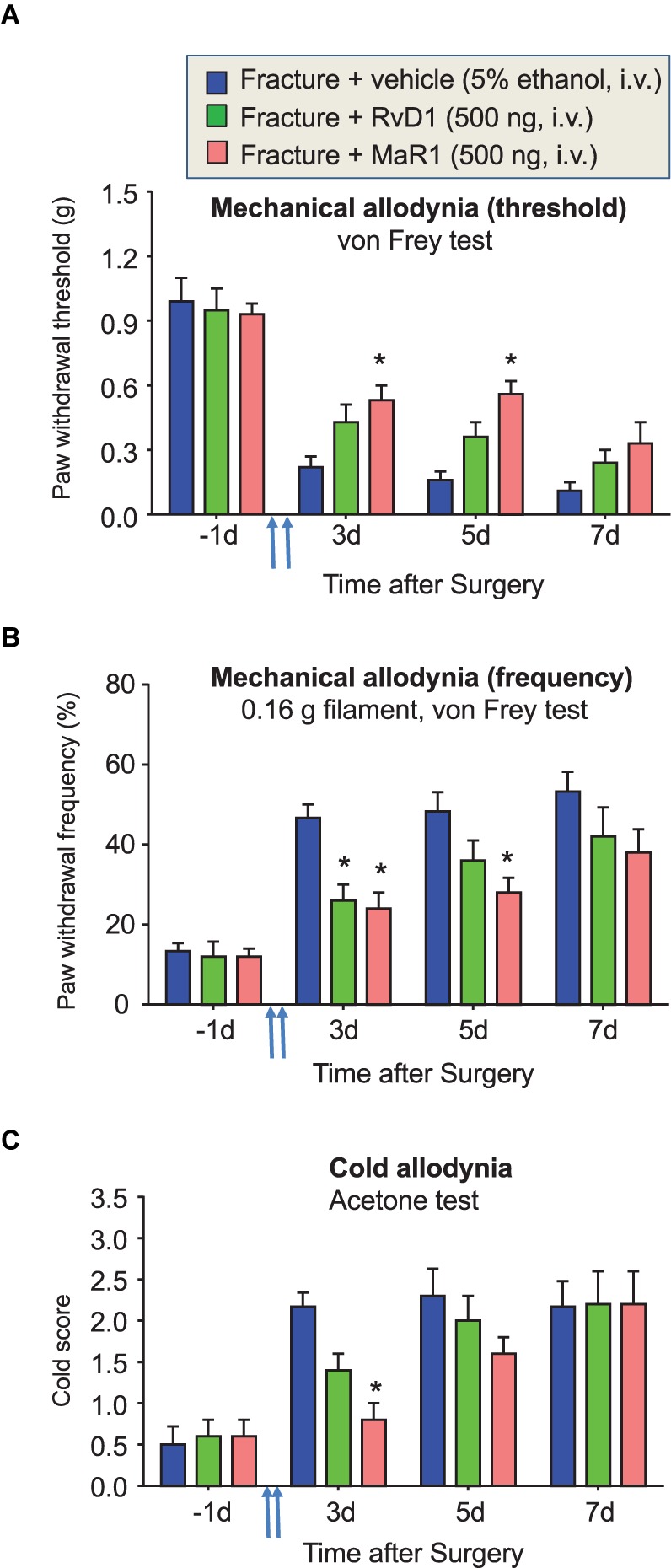
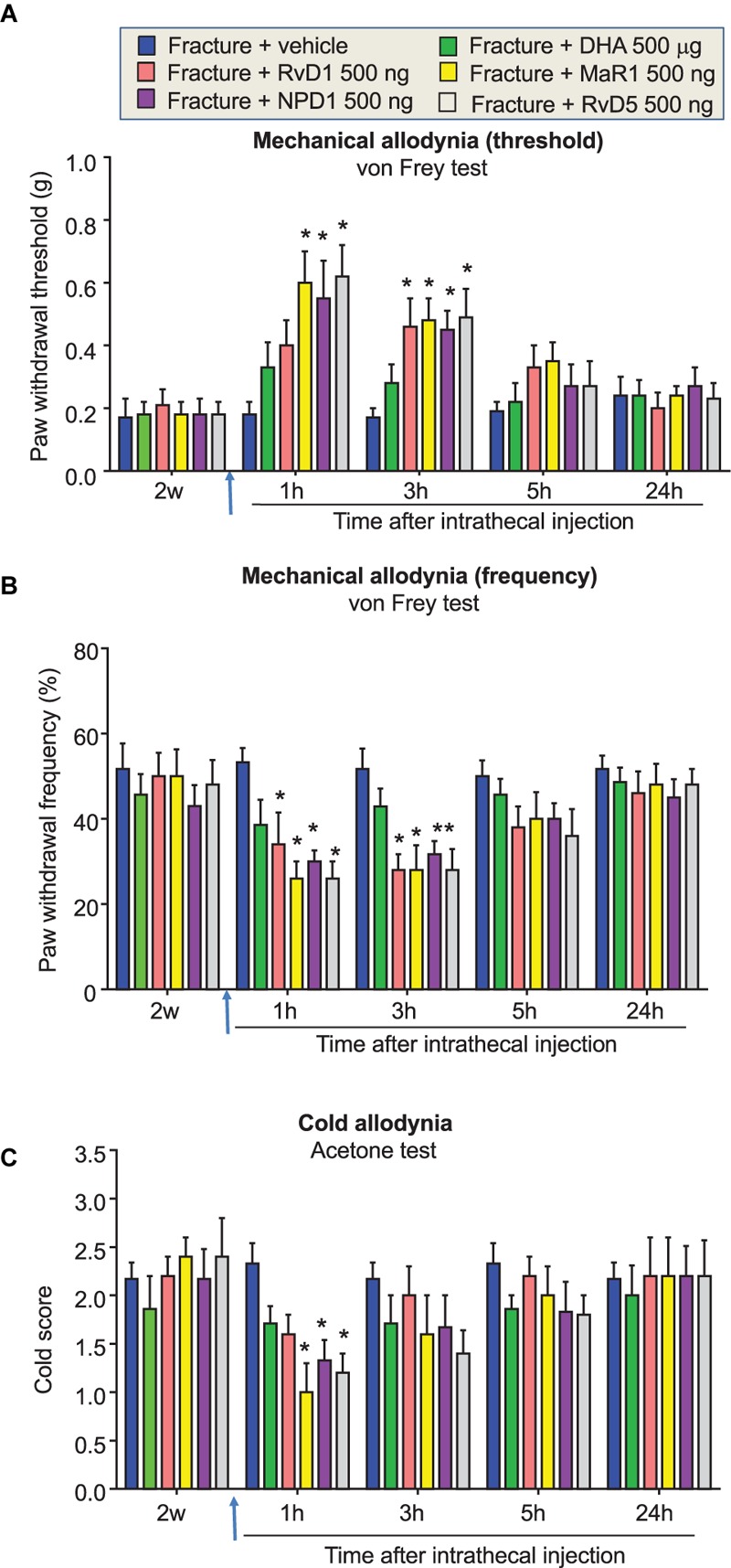
Mechanisms of pain resolution are largely unclear. Increasing evidence suggests that specialized pro-resolving mediators (SPMs), derived from fish oil docosahexaenoic acid (DHA), promote the resolution of acute inflammation and potently inhibit inflammatory and neuropathic pain. In this study, we examined the analgesic impact of DHA and DHA-derived SPMs in a mouse model of post-operative pain induced by tibial bone fracture (fPOP). Intravenous perioperative treatment with DHA (500 μg), resolvin D1 (RvD1, 500 ng) and maresin 1 (MaR1, 500 ng), 10 min and 24 h after the surgery, delayed the development of fPOP (mechanical allodynia and cold allodynia). In contrast, post-operative intrathecal (IT) administration of DHA (500 μg) 2 weeks after the surgery had no effects on established mechanical and cold allodynia. However, by direct comparison, IT post-operative treatment (500 ng) with neuroprotectin D1 (NPD1), MaR1, and D-resolvins, RvD1 and RvD5, but not RvD3 and RvD4, effectively reduced mechanical and cold allodynia. ELISA analysis showed that perioperative DHA treatment increased RvD1 levels in serum and spinal cord samples after bone fracture. Interestingly, sham surgery resulted in transient allodynia and increased RvD1 levels, suggesting a correlation of enhanced SPM levels with acute pain resolution after sham surgery. Our findings suggest that (1) perioperative treatment with DHA is effective in preventing and delaying the development of fPOP and (2) post-treatment with some SPMs can attenuate established fPOP. Our data also indicate that orthopedic surgery impairs SPM production. Thus, DHA and DHA-derived SPMs should be differentially supplemented for treating fPOP and improving recovery.
疼痛缓解的机制在很大程度上尚不清楚。越来越多的证据表明,源自鱼油二十二碳六烯酸(DHA)的特异性促炎症消退介质(SPM)可促进急性炎症的消退,并有效抑制炎性疼痛和神经性疼痛。在本研究中,我们在小鼠胫骨骨折诱导的术后疼痛(fPOP)模型中检测了DHA和源自DHA的SPM的镇痛作用。在手术后10分钟和24小时,静脉围手术期给予DHA(500μg)、消退素D1(RvD1,500ng)和maresin 1(MaR1,500ng),可延迟fPOP(机械性异常性疼痛和冷异常性疼痛)的发展。相比之下,术后2周鞘内注射(IT)DHA(500μg)对已确立的机械性和冷异常性疼痛没有影响。然而,通过直接比较,术后IT给予神经保护素D1(NPD1)、MaR1和D-消退素RvD1及RvD5(500ng),而非RvD3和RvD4,可有效减轻机械性和冷异常性疼痛。ELISA分析显示,围手术期DHA治疗可增加骨折后血清和脊髓样本中RvD1的水平。有趣的是,假手术导致短暂性异常性疼痛并使RvD1水平升高,提示增强的SPM水平与假手术后急性疼痛缓解相关。我们的研究结果表明:(1)围手术期给予DHA可有效预防和延迟fPOP的发展;(2)某些SPM的后期治疗可减轻已确立的fPOP。我们的数据还表明,骨科手术会损害SPM的产生。因此,应区别补充DHA和源自DHA的SPM来治疗fPOP并促进恢复。