Department of Anesthesia and Intensive Care, Neonatal and Pediatric Intensive Care Unit, Hospital Nord, Assistance-Publique des Hôpitaux de Marseille, 13015, Marseille, France.
Department of Neonatology, Hospital Nord, Assistance-Publique des Hôpitaux de Marseille, 13015, Marseille, France.
BMC Palliat Care. 2018 May 17;17(1):76. doi: 10.1186/s12904-018-0329-x.
Neonatal deaths are often associated with the complex decision to limit or withdraw life-sustaining interventions (LSIs) rather than therapeutic impasses. Despite the existence of a law, significant disparities in clinical procedures remain. This study aimed to assess deaths occurring in a Neonatal Intensive Care Unit (NICU) and measure the impact of a traceable Limitation or Withdrawal of Active Treatment (LWAT) file on the treatment of these newborns.
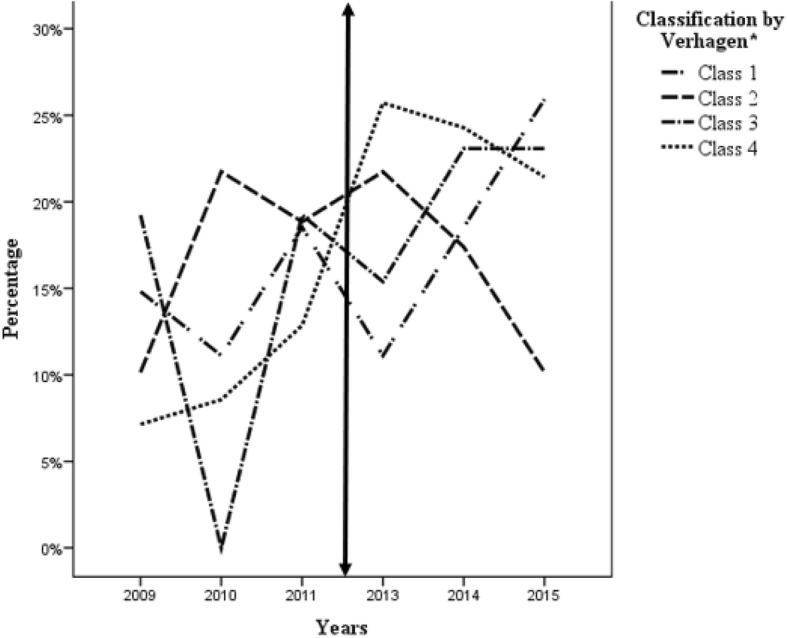
In this monocentric retrospective study, we reviewed all consecutive neonatal deaths occurring during two three-year periods among patients in the NICU at the North Hospital of Marseille: cohort 1 (from 2009 to 2011 without the LWAT file) and cohort 2 (from 2013 to 2015 after introduction of the LWAT file). Newborns included were: gestational age over 22 weeks, birth weight over 500 g, and admission and death in the same NICU. Deaths were categorized according to the classification described by Verhagen et al.: 1) children who died despite cardiopulmonary resuscitation (CPR) (no withholding nor withdrawing of LSIs), (2) children who died while the ventilator, without CPR (no withdrawing of LSIs, but CPR withheld), (3) children who died after LSIs were withdrawn, or (4) LSIs were withheld.
193 deaths were analyzed: 77 in cohort 1 and 116 in cohort 2. 50% of deaths followed the decision to limit or stop life-sustaining interventions. The mean age at death did not differ between the two cohorts (p = 0.525). An increase in the mortality rate after life-sustaining interventions were withdrawn was observed. The number of multidisciplinary decision meetings was statistically higher in cohort 2 (32.5% versus 55.2% p = 0.002), which were most often prompted due to neurological pathologies, with an increase in parental advice concerning the management of their child (p = 0.026). Even if the introduction of this file did not have an effect on patient age at death, it was significantly associated with a better understanding of end-of-life conditions (p = 0.019), including medication used to sedate and comfort the patient.
Introduction of the LWAT file seems imperative to develop a personalized healthcare strategy for each child and situation.
新生儿死亡通常与限制或停止维持生命的干预措施(LSI)的复杂决策有关,而不是与治疗僵局有关。尽管存在法律,但临床程序仍存在显著差异。本研究旨在评估新生儿重症监护病房(NICU)中的死亡情况,并衡量可追踪的限制或停止主动治疗(LWAT)文件对这些新生儿治疗的影响。
在这项单中心回顾性研究中,我们回顾了马赛北部医院 NICU 中连续两个三年期间发生的所有新生儿死亡病例:队列 1(2009 年至 2011 年,无 LWAT 文件)和队列 2(2013 年至 2015 年,引入 LWAT 文件后)。纳入的新生儿为:胎龄超过 22 周,出生体重超过 500 克,在同一 NICU 入院和死亡。死亡根据 Verhagen 等人描述的分类进行分类:1)尽管进行了心肺复苏(CPR)但仍死亡的儿童(未停止 LSI),2)在没有 CPR 的情况下呼吸机死亡的儿童(未停止 LSI,但停止 CPR),3)停止 LSI 后死亡的儿童,或 4)停止 LSI。
共分析了 193 例死亡病例:队列 1 77 例,队列 2 116 例。50%的死亡是由于决定限制或停止维持生命的干预措施。两组之间的死亡年龄无差异(p=0.525)。在停止维持生命的干预措施后,死亡率有所增加。在队列 2 中,多学科决策会议的数量统计上更高(32.5%比 55.2%,p=0.002),这些会议主要是由于神经病理学引起的,与增加对父母关于管理其孩子的建议(p=0.026)。尽管引入该文件对患者的死亡年龄没有影响,但它与更好地了解生命末期的情况显著相关(p=0.019),包括用于镇静和安慰患者的药物。
引入 LWAT 文件似乎对于为每个孩子和情况制定个性化的医疗保健策略至关重要。