Department of Intensive Care Medicine, Ghent University Hospital, Corneel Heymanslaan 10, Ghent, Belgium.
Department of Intensive Care Medicine, Vejle Hospital, Vejle, Denmark.
Intensive Care Med. 2018 Jul;44(7):1039-1049. doi: 10.1007/s00134-018-5231-8. Epub 2018 May 28.
Whether the quality of the ethical climate in the intensive care unit (ICU) improves the identification of patients receiving excessive care and affects patient outcomes is unknown.
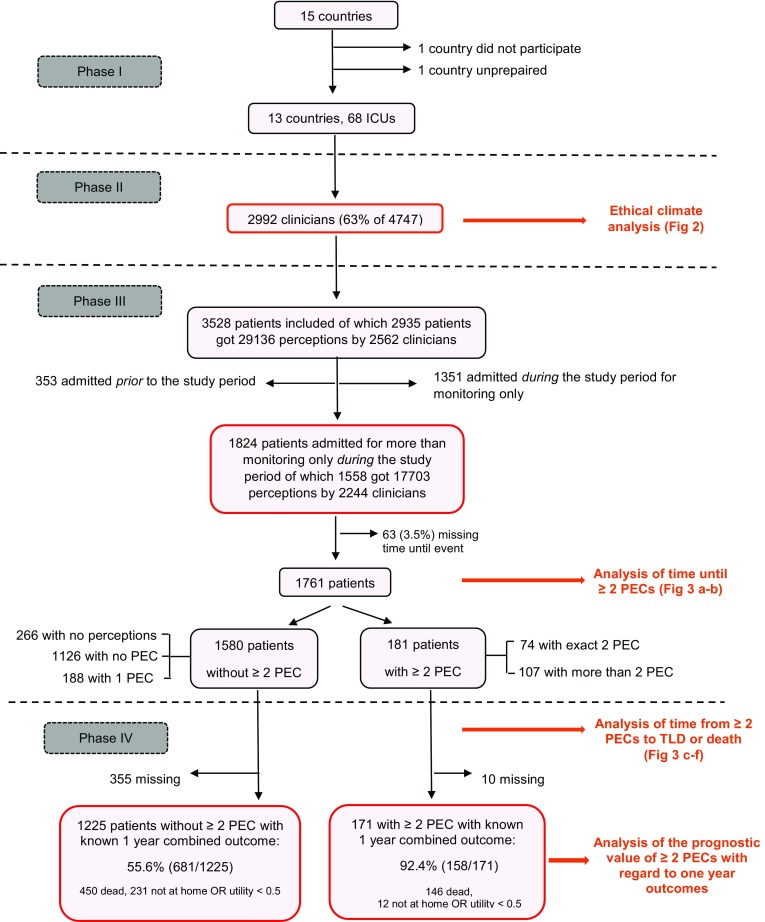
In this prospective observational study, perceptions of excessive care (PECs) by clinicians working in 68 ICUs in Europe and the USA were collected daily during a 28-day period. The quality of the ethical climate in the ICUs was assessed via a validated questionnaire. We compared the combined endpoint (death, not at home or poor quality of life at 1 year) of patients with PECs and the time from PECs until written treatment-limitation decisions (TLDs) and death across the four climates defined via cluster analysis.
Of the 4747 eligible clinicians, 2992 (63%) evaluated the ethical climate in their ICU. Of the 321 and 623 patients not admitted for monitoring only in ICUs with a good (n = 12, 18%) and poor (n = 24, 35%) climate, 36 (11%) and 74 (12%), respectively were identified with PECs by at least two clinicians. Of the 35 and 71 identified patients with an available combined endpoint, 100% (95% CI 90.0-1.00) and 85.9% (75.4-92.0) (P = 0.02) attained that endpoint. The risk of death (HR 1.88, 95% CI 1.20-2.92) or receiving a written TLD (HR 2.32, CI 1.11-4.85) in patients with PECs by at least two clinicians was higher in ICUs with a good climate than in those with a poor one. The differences between ICUs with an average climate, with (n = 12, 18%) or without (n = 20, 29%) nursing involvement at the end of life, and ICUs with a poor climate were less obvious but still in favour of the former.
Enhancing the quality of the ethical climate in the ICU may improve both the identification of patients receiving excessive care and the decision-making process at the end of life.
在重症监护病房(ICU)中,伦理氛围的质量是否能够改善对过度治疗患者的识别,并影响患者的结局,目前尚不清楚。
本前瞻性观察性研究在欧洲和美国的 68 家 ICU 中,连续 28 天每天收集临床医生对过度治疗(PECs)的看法。通过经过验证的问卷评估 ICU 中的伦理氛围质量。我们比较了有 PECs 的患者的综合终点(死亡、不在家或 1 年后生活质量差)以及从 PECs 到书面治疗限制决定(TLDs)和死亡的时间,这是通过聚类分析定义的四个气候组的差异。
在 4747 名符合条件的临床医生中,有 2992 名(63%)评估了其 ICU 的伦理氛围。在监测仅在伦理氛围良好(n=12,18%)和差(n=24,35%)的 ICU 中不接受治疗的 321 名和 623 名患者中,分别有 36 名(11%)和 74 名(12%)患者被至少两名临床医生识别出有 PECs。在 35 名和 71 名有可用综合终点的患者中,分别有 100%(95%CI 90.0-1.00)和 85.9%(75.4-92.0)(P=0.02)达到该终点。在至少两名临床医生有 PECs 的患者中,在 ICU 中,良好的伦理氛围与较差的伦理氛围相比,死亡风险(HR 1.88,95%CI 1.20-2.92)或获得书面 TLD(HR 2.32,CI 1.11-4.85)的风险更高。在 ICU 中,平均气候(n=12,18%)或无护理参与(n=20,29%)与较差气候之间的差异不太明显,但仍有利于前者。
提高 ICU 的伦理氛围质量可能会改善对过度治疗患者的识别,以及临终决策过程。