Department of Internal Diseases “Prof. St. Kirkovich”, Medical University of Sofia, Bulgaria
Balkan Med J. 2018 May 29;35(3):233-237. doi: 10.4274/balkanmedj.2017.0580.
Pericardial effusion in chronic hypoxemic lung diseases, such as Obstructive Sleep Apnea syndrome, usually occurs after the development of severe pulmonary arterial hypertension. However, data about the frequency of pericardial effusions in Obstructive Sleep Apnea syndrome without pulmonary arterial hypertension and/or daytime hypoxemia are still scarce, and their pathogenesis is unclear.
To assess the prevalence of pericardial effusions and their volume and location in patients with obesity and Obstructive Sleep Apnea syndrome without pulmonary arterial hypertension and/or hypoxemia.
Cross-sectional study.
We included 279 consecutive patients (162 males) with newly diagnosed Obstructive Sleep Apnea syndrome having a mean age of 42.8±12.4 years and a mean body mass index of 37.3±7.8 kg/m2. Obstructive Sleep Apnea syndrome was confirmed by polysomnography. Main exclusion criteria were concomitant inflammatory diseases, thyroid dysfunction, daytime hypoxemia, nephrotic syndrome, left ventricular systolic dysfunction and pulmonary arterial hypertension.
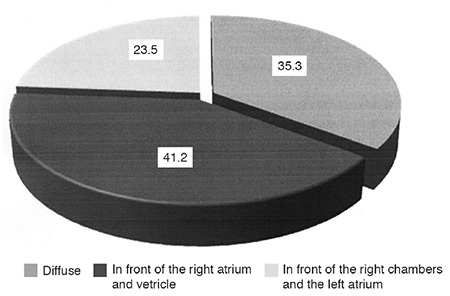
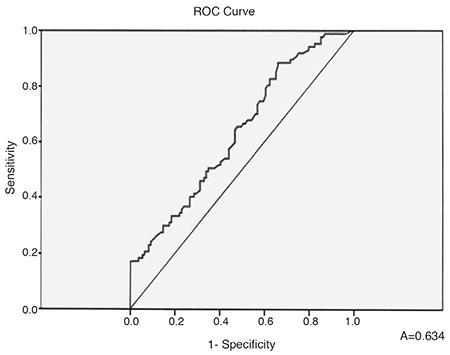
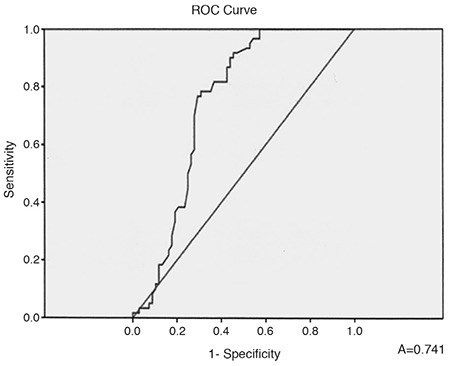
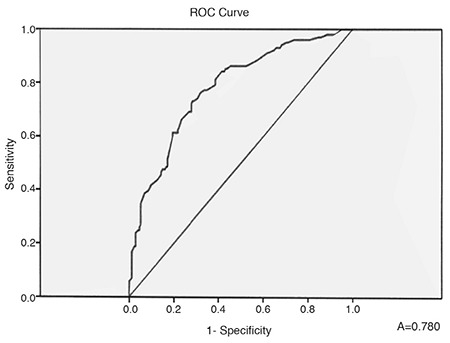
Pericardial effusion was found in 102 (36.56%) -all of them with moderate to severe obstructive Sleep Apnea syndrome. The mean effusion volume was mild to moderate (up to 250 mL). In 36 patients (35.3%) the pericardial effusion was diffuse, in 42 (41.2%), the pericardial effusion was located in front of the right atrium and the right ventricle, and in 24 (23.5%) the pericardial effusion was situated in front of the right cardiac cavities and the left atrium. We found a significant positive correlation between the presence of pericardial effusion and apnea-hypopnea index (r=0.374, p<0.001), body mass index (r=0.473, p<0.001), and desaturation time during sleep (r=0.289, p<0.001).
Pericardial effusion in patients with obesity and moderate to severe Obstructive Sleep Apnea syndrome without daily hypoxemia and/or pulmonary hypertension is a relatively common finding. The occurrence of pericardial effusions is dependent mostly on the grade of Obstructive Sleep Apnea syndrome, degree of obesity, and duration of sleep desaturation.
在慢性低氧性肺部疾病(如阻塞性睡眠呼吸暂停综合征)中,心包积液通常发生在严重肺动脉高压之后。然而,关于无肺动脉高压和/或日间低氧血症的阻塞性睡眠呼吸暂停综合征患者中心包积液的发生频率的数据仍然很少,其发病机制尚不清楚。
评估肥胖症和无肺动脉高压和/或低氧血症的阻塞性睡眠呼吸暂停综合征患者心包积液的发生率及其容量和位置。
横断面研究。
我们纳入了 279 例新诊断为阻塞性睡眠呼吸暂停综合征的连续患者(162 例男性),平均年龄为 42.8±12.4 岁,平均体重指数为 37.3±7.8kg/m2。阻塞性睡眠呼吸暂停综合征通过多导睡眠图确认。主要排除标准为合并炎症性疾病、甲状腺功能减退症、日间低氧血症、肾病综合征、左心室收缩功能障碍和肺动脉高压。
102 例(36.56%)患者存在心包积液-均为中重度阻塞性睡眠呼吸暂停综合征。心包积液平均量为轻度至中度(达 250mL)。36 例(35.3%)患者的心包积液为弥漫性,42 例(41.2%)患者的心包积液位于右心房和右心室前方,24 例(23.5%)患者的心包积液位于右心腔和左心房前方。我们发现心包积液的存在与呼吸暂停-低通气指数(r=0.374,p<0.001)、体重指数(r=0.473,p<0.001)和睡眠期间的低氧时间(r=0.289,p<0.001)之间存在显著正相关。
肥胖症和中重度阻塞性睡眠呼吸暂停综合征患者,无日间低氧血症和/或肺动脉高压,心包积液是一种相对常见的发现。心包积液的发生主要取决于阻塞性睡眠呼吸暂停综合征的严重程度、肥胖程度和睡眠低氧时间。