VA Center for Clinical Management Research and University of Michigan Medical School, Ann Arbor, Michigan (T.J.C., R.A.H.).
University of Michigan, Ann Arbor, Michigan (P.C., R.M.).
Ann Intern Med. 2018 Jul 3;169(1):1-9. doi: 10.7326/M17-2561. Epub 2018 May 29.
Many health systems are exploring how to implement low-dose computed tomography (LDCT) screening programs that are effective and patient-centered.
To examine factors that influence when LDCT screening is preference-sensitive.
State-transition microsimulation model.
Two large randomized trials, published decision analyses, and the SEER (Surveillance, Epidemiology, and End Results) cancer registry.
U.S.-representative sample of simulated patients meeting current U.S. Preventive Services Task Force criteria for screening eligibility.
Lifetime.
Individual.
LDCT screening annually for 3 years.
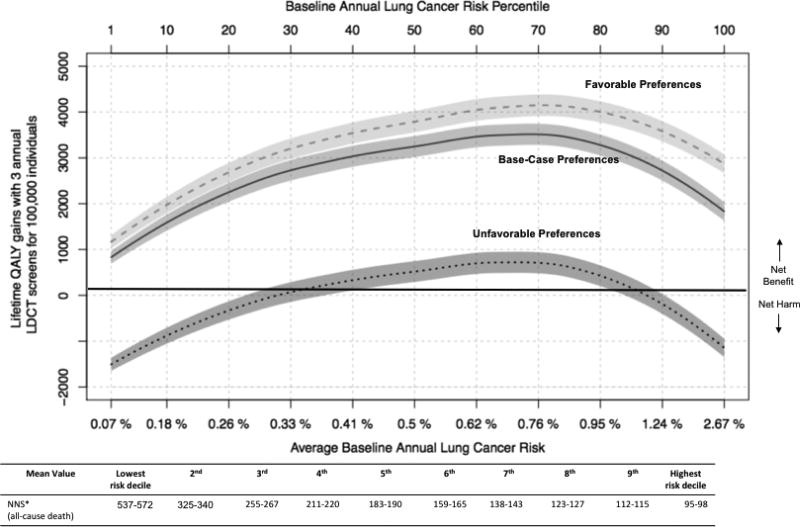
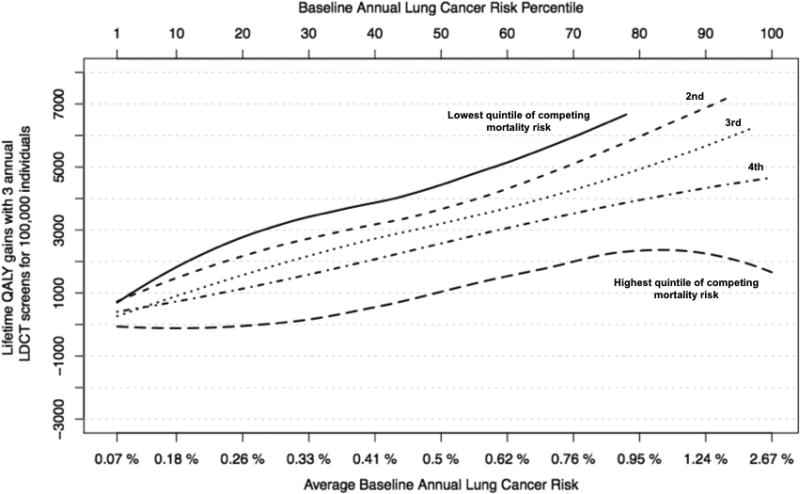
Lifetime quality-adjusted life-year gains and reduction in lung cancer mortality. To examine the effect of preferences on net benefit, disutilities (the "degree of dislike") quantifying the burden of screening and follow-up were varied across a likely range. The effect of varying the rate of false-positive screening results and overdiagnosis associated with screening was also examined.
RESULTS OF BASE-CASE ANALYSIS: Moderate differences in preferences about the downsides of LDCT screening influenced whether screening was appropriate for eligible persons with annual lung cancer risk less than 0.3% or life expectancy less than 10.5 years. For higher-risk eligible persons with longer life expectancy (roughly 50% of the study population), the benefits of LDCT screening overcame even highly negative views about screening and its downsides.
Rates of false-positive findings and overdiagnosed lung cancer were not highly influential.
The quantitative thresholds that were identified may vary depending on the structure of the microsimulation model.
Identifying circumstances in which LDCT screening is more versus less preference-sensitive may help clinicians personalize their screening discussions, tailoring to both preferences and clinical benefit.
None.
许多医疗系统正在探索如何实施有效且以患者为中心的低剂量计算机断层扫描(LDCT)筛查计划。
研究影响 LDCT 筛查偏好敏感性的因素。
状态转换微模拟模型。
两项大型随机试验、已发表的决策分析以及 SEER(监测、流行病学和最终结果)癌症登记处。
符合当前美国预防服务工作组筛查资格标准的模拟患者的美国代表性样本。
终生。
个体。
每年进行 LDCT 筛查 3 年。
终生质量调整生命年的获益和肺癌死亡率的降低。为了研究偏好对净效益的影响,我们在可能的范围内改变了量化筛查和随访负担的不舒适(“厌恶程度”)的贴现率。还研究了改变与筛查相关的假阳性筛查结果和过度诊断率的影响。
对 LDCT 筛查不利方面的偏好差异会影响每年肺癌风险低于 0.3%或预期寿命低于 10.5 年的合格人员是否适合进行筛查。对于预期寿命较长(约占研究人群的 50%)、风险较高的合格人员,LDCT 筛查的益处甚至可以克服对筛查及其不利方面的高度负面看法。
假阳性发现率和过度诊断的肺癌率并没有很大的影响。
确定的定量阈值可能因微模拟模型的结构而异。
确定 LDCT 筛查更具偏好敏感性而非敏感性的情况可能有助于临床医生个性化他们的筛查讨论,既考虑到偏好,又考虑到临床获益。
无。