Morton Rachael L, Schlackow Iryna, Gray Alastair, Emberson Jonathan, Herrington William, Staplin Natalie, Reith Christina, Howard Kirsten, Landray Martin J, Cass Alan, Baigent Colin, Mihaylova Borislava
NHMRC Clinical Trials Centre, The University of Sydney, Sydney, Australia.
Health Economics Research Centre, Nuffield Department of Population Health, University of Oxford, UK.
Kidney Int Rep. 2017 Dec 23;3(3):610-618. doi: 10.1016/j.ekir.2017.12.008. eCollection 2018 May.
The impact of chronic kidney disease (CKD) on income is unclear. We sought to determine whether CKD severity, serious adverse events, and CKD progression affected household income.
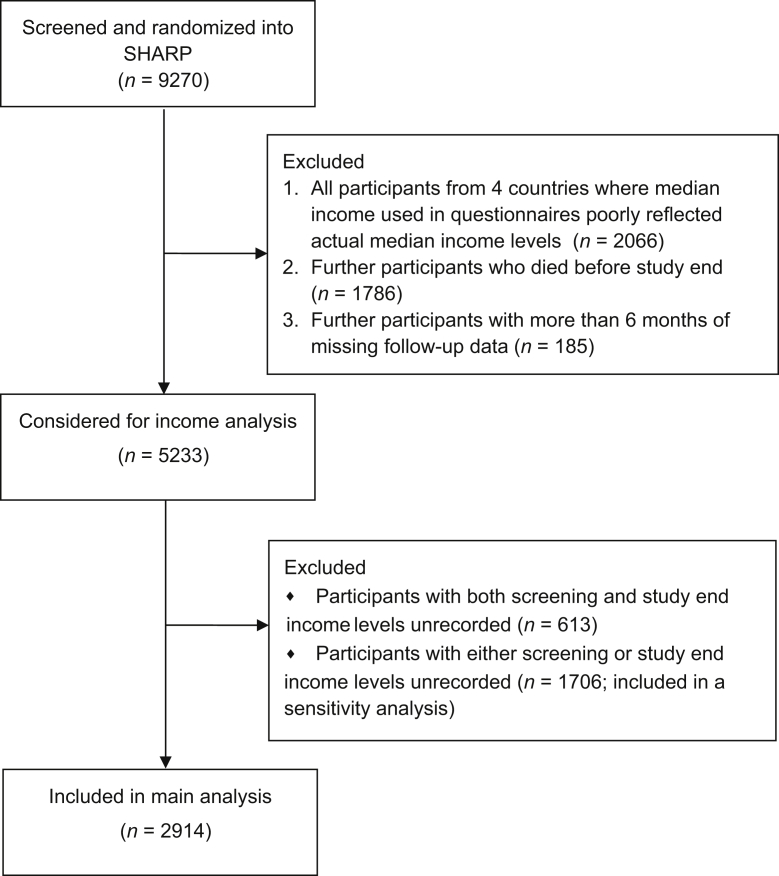
Analyses were undertaken in a prospective cohort of adults with moderate-to-severe CKD in the Study of Heart and Renal Protection (SHARP), with household income information available at baseline screening and study end. Logistic regressions, adjusted for sociodemographic characteristics, smoking, and prior diseases at baseline, estimated associations during the 5-year follow-up, among (i) baseline CKD severity, (ii) incident nonfatal serious adverse events (vascular or cancer), and (iii) CKD treatment modality (predialysis, dialysis, or transplanted) at study end and the outcome "fall into relative poverty." This was defined as household income <50% of country median income.
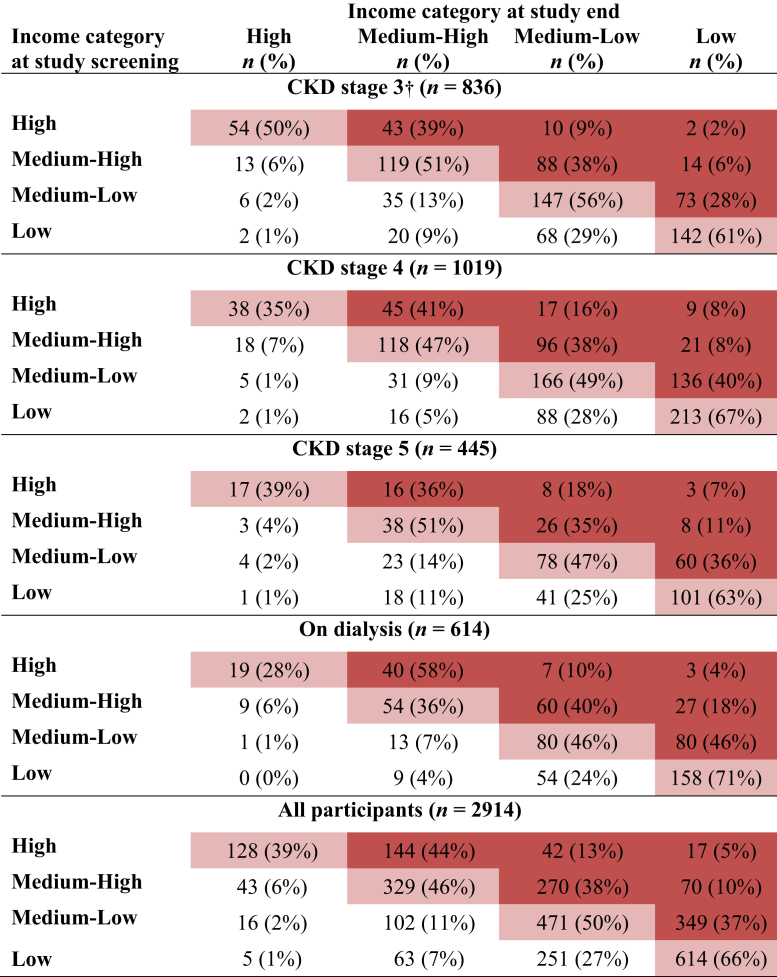
A total of 2914 SHARP participants from 14 countries were included in the main analysis. Of these, 933 (32%) were in relative poverty at screening; of the remaining 1981, 436 (22%) fell into relative poverty by study end. Compared with participants with stage 3 CKD at baseline, the odds of falling into poverty were 51% higher for those with stage 4 (odds ratio [OR]: 1.51; 95% confidence interval [CI]: 1.09-2.10), 66% higher for those with stage 5 (OR: 1.66; 95% CI: 1.11-2.47), and 78% higher for those on dialysis at baseline (OR: 1.78, 95% CI: 1.22-2.60). Participants with kidney transplant at study end had approximately half the risk of those on dialysis or those with CKD stages 3 to 5.
More advanced CKD is associated with increased odds of falling into poverty. Kidney transplantation may have a role in reducing this risk.
慢性肾脏病(CKD)对收入的影响尚不清楚。我们试图确定CKD的严重程度、严重不良事件和CKD进展是否会影响家庭收入。
在心脏和肾脏保护研究(SHARP)中,对患有中度至重度CKD的成年人前瞻性队列进行分析,在基线筛查和研究结束时可获得家庭收入信息。在对社会人口学特征、吸烟情况和基线时的既往疾病进行校正后,通过逻辑回归估计在5年随访期间,(i)基线CKD严重程度、(ii)非致命性严重不良事件(血管性或癌症)、(iii)研究结束时的CKD治疗方式(透析前、透析或移植)与“陷入相对贫困”这一结果之间的关联。“陷入相对贫困”定义为家庭收入低于国家收入中位数的50%。
主要分析纳入了来自14个国家的2914名SHARP参与者。其中,933名(32%)在筛查时处于相对贫困状态;在其余1981名参与者中,436名(22%)在研究结束时陷入相对贫困。与基线时患有3期CKD的参与者相比,4期患者陷入贫困的几率高51%(比值比[OR]:1.51;95%置信区间[CI]:1.09 - 2.10),5期患者高66%(OR:1.66;95%CI:1.11 - 2.47),基线时接受透析的患者高78%(OR:1.78,95%CI:1.22 - 2.60)。研究结束时接受肾移植的参与者陷入贫困的风险约为接受透析者或CKD 3至5期患者的一半。
更晚期的CKD与陷入贫困的几率增加相关。肾移植可能在降低这种风险方面发挥作用。