Amol S. Navathe (
Joshua M. Liao is an assistant professor in the Department of Medicine at the University of Washington School of Medicine, in Seattle.
Health Aff (Millwood). 2018 Jun;37(6):854-863. doi: 10.1377/hlthaff.2017.1358.
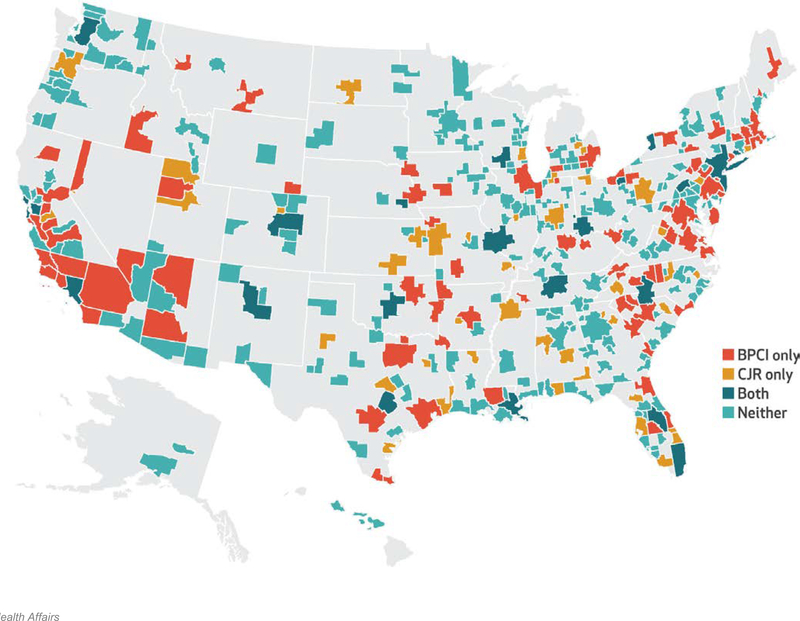
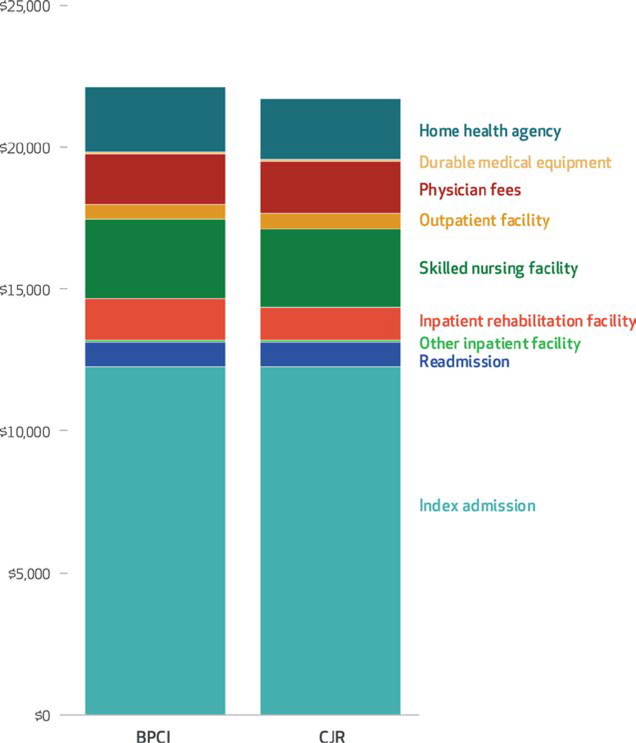
We analyzed data from Medicare and the American Hospital Association Annual Survey to compare characteristics and baseline performance among hospitals in Medicare's voluntary (Bundled Payments for Care Improvement initiative, or BPCI) and mandatory (Comprehensive Care for Joint Replacement Model, or CJR) joint replacement bundled payment programs. BPCI hospitals had higher mean patient volume and were larger and more teaching intensive than were CJR hospitals, but the two groups had similar risk exposure and baseline episode quality and cost. BPCI hospitals also had higher cost attributable to institutional postacute care, largely driven by inpatient rehabilitation facility cost. These findings suggest that while both voluntary and mandatory approaches can play a role in engaging hospitals in bundled payment, mandatory programs can produce more robust, generalizable evidence. Either mandatory or additional targeted voluntary programs may be required to engage more hospitals in bundled payment programs.
我们分析了医疗保险和美国医院协会年度调查的数据,以比较医疗保险自愿性(捆绑支付改善护理计划,或 BPCI)和强制性(关节置换综合护理模式,或 CJR)关节置换捆绑支付计划中医院的特征和基线绩效。BPCI 医院的平均患者量较高,规模较大,教学强度较高,而 CJR 医院则风险暴露、基线发病质量和成本相似。BPCI 医院的机构后期护理成本也较高,主要是由于住院康复设施成本较高。这些发现表明,虽然自愿和强制方法都可以在捆绑支付方面发挥作用,但强制方案可以产生更强大、更具普遍性的证据。可能需要强制性或额外的有针对性的自愿方案来让更多的医院参与捆绑支付计划。